Does anyone know the percentage of actual testosterone that's in each ester? I'm having a hard time finding any conclusive numbers. I'm switching over to propionate, from cypionate, and would just like to know how to do the conversion. I can figure that part out once I have the percentages of testosterone in each ester. Thanks.
ANABOLICS 10ed by Llewellyn
Esters and Injectable Compounds
You may notice that many injectable steroids will list long chemical names like testosterone cypionate and testosterone enanthate, instead of just testosterone. In these cases, the cypionate and enanthate are esters (carboxylic acids) that have been attached to the 17-beta hydroxyl group of the testosterone molecule, which increase the active life span of the steroid preparation. Such alterations will reduce the steroid's level of water solubility, and increase its oil solubility. Once an esterified compound has been injected, it will form a deposit in the muscle tissue (depot) from which it will slowly enter circulation. Generally the larger the ester chain, the more oil soluble the steroid compound will be, and the longer it will take for the full dosage to be released.
Once free in circulation, enzymes will quickly remove the ester chain and the parent hormone will be free to exert its activity (while the ester is present the steroid is inert).
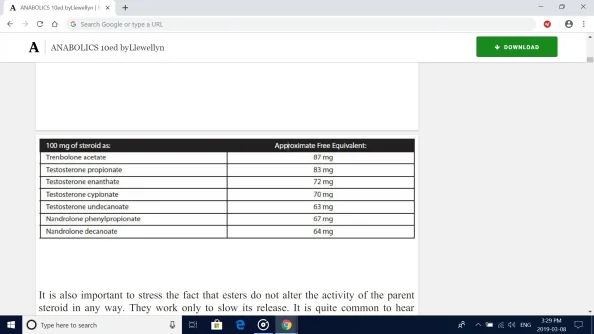
There are a wide number of esters, which can provide varying release times, used in medicine today. To compare, an ester like decanoate can extend the release of active parent drug into the blood stream for three to four weeks, while it may only be extended for a few days with an acetate or propionate ester. The use of an ester allows for a much less frequent injection schedule than if using a water-based (straight) testosterone, which is much more comfortable for the patient. We must remember when calculating dosages, that the ester is figured into the steroid's measured weight.100 mg of testosterone enanthate, therefore, contains much less base hormone than 100 mg of a straight testosterone suspension (in this case it equals 72 mg of testosterone).
In some instances, an ester may account for roughly 40% or more of the total steroid weight, but the typical measure is somewhere around 15% to 35%. Below are the free base equivalents for several popular steroid compounds.
It is also important to stress the fact that esters do not alter the activity of the parent steroid in any way. They work only to slow its release. It is quite common to hear people speak about the properties of different esters,
almost as if they can magically alter a steroid's effectiveness. This is really nonsense. Enanthate is not more powerful than cypionate (perhaps a few extra milligrams of testosterone released per injection, but nothing to note), nor is Sustanon some type of incredible testosterone blend.Personally, I have always considered Sustanon a very poor buy in the face of cheaper 250 mg enanthate ampules. Your muscle cells see only testosterone; ultimately there is no difference.
Reports of varying levels of muscle gain, androgenic side effects, water retention, etc. are only issues of timing. Faster releasing testosterone esters will produce estrogen build up faster simply because there is more testosterone free in the blood from the start of the cycle. The same is true when we state that Durabolin® is amilder nandrolone for women compared to Deca. It is simply easier to control the blood level with a faster acting drug. Were virilization symptoms to become apparent,hormone levels will drop much faster once we stop administration. This should not be confused with the notion that the nandrolone in Durabolin® acts differently in the body than that released from a shot of Deca-Durabolin®.
It is also worth noting that while the
ester is typically hydrolyzed in general circulation, some will be hydrolyzed at the injection site where the steroid depot first contacts blood. This will cause a slightly higher concentration of both free steroid and ester in the muscle where the drug had been administered. On the plus side, this may equate to slightly better growth in this muscle, as more hormone is made available to nearby cells. Many bodybuilders have come to swear by the use of injection sites such as the deltoids, biceps, and triceps, truly believing better growth can be achieved if the steroid is injected directly into these muscles.
The negative to this is that the ester itself may be irritating to the tissues at the site of injection once it is broken free. In some instances it can be so caustic that the muscle itself will become swollen and sore due to the presence of the ester, and the user may even suffer a low grade fever as the body fights off the irritant (the onset of such symptoms typically occurs 24-72 hours after injection). This effect is more common with small chain esters such as propionate and acetate, and can actually make a popular steroid such as Sustanon (which contains testosterone propionate) off-limits for some users who experience too much discomfort to justify using the drug. Longer chain esters such as decanoate and cypionate are typically much less irritating at the site of injection, and therefore are preferred by sensitive individuals.