Debunking the Myth About High Hematocrit in Men on TRT
I know many of you want to feel reassured that managing hematocrit isn’t necessary. However, misinformation is spreading, with some "bro science" videos and even a few so-called expert doctors claiming that men on TRT don’t need to worry about elevated hematocrit because people living at high altitudes have high hematocrit without increased mortality.
Let’s set the record straight—again.
High hematocrit in men on TRT is NOT the same as high hematocrit in people living at high altitudes. These are two completely different physiological conditions. Here’s why:
- TRT Increases Both Hematocrit and Blood Volume
- Testosterone stimulates red blood cell production, raising hematocrit.
- It also increases blood volume due to sodium retention and other factors.
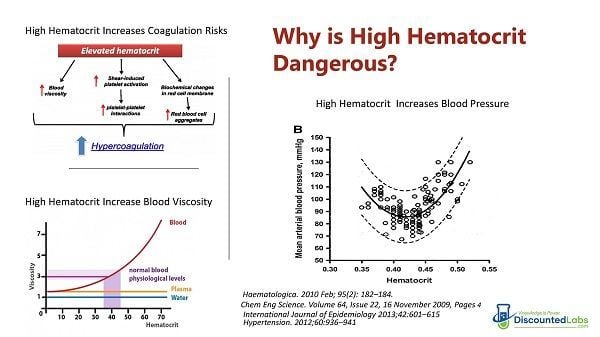
- This combination can contribute to increased blood viscosity, which raises cardiovascular risk.
- People at High Altitudes Experience Different Physiological Adaptations
- At high altitudes, lower oxygen availability triggers an increase in red blood cell production to compensate.
- However, these individuals do not experience the same increase in blood volume that men on TRT do.
- Additionally, hypoxia (low oxygen levels) promotes blood vessel dilation, helping maintain proper circulation despite increased hematocrit.
A key paper on altitude physiology states:
"To compensate for the low partial pressure of oxygen at altitude, the body undergoes physiological changes, including increased circulating hemoglobin. However, there is also a fall in plasma volume, increasing hemoglobin concentration in the early stages of hypoxic exposure."
The crucial difference? Men on TRT experience increased blood viscosity due to both higher hematocrit AND increased blood volume, while high-altitude dwellers do not.
The Data on TRT, High Hematocrit, and Cardiovascular Risk
Real-world evidence is already showing that elevated hematocrit in men on TRT is linked to a higher risk of cardiovascular events. For example:
Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy: A Retrospective Cohort Claims Database Analysis.
This study found a significant correlation between increased hematocrit and cardiovascular risks in men undergoing TRT.

Conclusion
The claim that men on TRT with high hematocrit face no additional health risks because high-altitude residents have high hematocrit is scientifically flawed. These are two different conditions with fundamentally different effects on blood circulation and cardiovascular health.
If you are on TRT and your hematocrit is rising significantly, it is not something to ignore. Proper monitoring and management are essential for long-term health.
People living at high altitudes who have high hematocrit are NOT the same as men on TRT with high hematocrit who live at "normal" altitudes. Why?
TRT increases red blood cells/hematocrit AND blood volume (due to sodium retention and other factors) AND blood pressure (depending on the patient). People at high altitudes (and not on TRT) are exposed to lower atmospheric partial pressures, which increases dilation of blood vessels. These people also do not experience increased blood volume even with higher red blood cells/hematocrit.
"In order to compensate for the low partial pressure of oxygen at altitude, the human body undergoes a number of physiological changes. A vital component in this process is the increase in the concentration of circulating hemoglobin. The role of HIF-1alpha, erythropoietin and red blood cells in this acclimatization process is described, together with the fall in plasma volume that increases the concentration of hemoglobin in the early stages of hypoxic exposure."
Difference between these people and men on TRT: We have increased blood volume and hemoglobin/hematocrit.
Full paper: Heights and haematology: the story of haemoglobin at altitude
We already are gathering data on higher mortality in men on TRT who have high hematocrit:
Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy: A Retrospective Cohort Claims Database Analysis
___________________________________________
Why is managing hematocrit important for men on TRT?
Managing hematocrit is crucial for men on Testosterone Replacement Therapy (TRT) because elevated hematocrit, when combined with increased blood volume due to TRT, leads to higher blood viscosity. This increased viscosity raises the risk of cardiovascular events, including major adverse cardiovascular events. It's a significant health concern that requires proper monitoring and management.How does high hematocrit in men on TRT differ from high hematocrit in people at high altitudes?
High hematocrit in men on TRT is physiologically distinct from high hematocrit in people living at high altitudes. While both conditions involve an increase in red blood cell production, TRT also causes an increase in blood volume due to sodium retention and other factors. This combination significantly increases blood viscosity. In contrast, people at high altitudes experience lower oxygen availability, which stimulates red blood cell production, but they do not experience the same increase in blood volume. Additionally, hypoxia (low oxygen levels) at high altitudes promotes blood vessel dilation, helping to maintain proper circulation despite increased hematocrit.What are the specific physiological differences between TRT-induced high hematocrit and altitude-induced high hematocrit?
The key physiological differences are:- TRT-induced: Testosterone stimulates red blood cell production (raising hematocrit) AND increases blood volume (due to sodium retention). This leads to increased blood viscosity and potentially higher blood pressure.
- Altitude-induced: Lower oxygen availability triggers increased red blood cell production. However, these individuals typically experience a fall in plasma volume, which helps to increase hemoglobin concentration without a significant increase in overall blood volume. Hypoxia also promotes blood vessel dilation, aiding circulation.
Is there scientific evidence linking elevated hematocrit in men on TRT to cardiovascular risk?
Yes, real-world evidence strongly suggests a link. Studies, such as "Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy: A Retrospective Cohort Claims Database Analysis," have found a significant correlation between increased hematocrit and cardiovascular risks in men undergoing TRT. This contradicts the misconception that TRT-induced high hematocrit is benign.What is the mechanism by which testosterone increases hematocrit?
Testosterone stimulates erythropoiesis (red blood cell production) through several mechanisms. Primarily, it causes an initial rise in erythropoietin (EPO), establishes a new EPO/hemoglobin 'set point,' and leads to a parallel decrease in hepcidin, a master iron regulator protein. Additionally, testosterone is transported into cells, particularly in the kidneys, by SHBG binding to megalin, which further explains its significant effect on EPO production.Why should men on TRT be skeptical of "Internet gurus" or certain doctors downplaying the risks of high hematocrit?
Men on TRT should be highly skeptical of individuals, especially those primarily motivated by financial gain (e.g., in podcasts or YouTube videos), who claim that managing hematocrit on TRT is unnecessary. This misinformation, often referred to as "bro science," ignores the fundamental physiological differences between TRT-induced erythrocytosis and high-altitude adaptation, as well as the scientific evidence linking high hematocrit on TRT to increased cardiovascular risk. Many of these sources also lack a deep understanding of the complex biological mechanisms involved.What is considered a "high" hematocrit level for men on TRT, and why is it important to monitor?
While specific numbers can vary, a hematocrit level over 54% is often considered high and warrants concern. Some sources suggest that levels above 55% are seen regularly in online groups, with some even reaching 60%. It's crucial to monitor because the problems associated with elevated hematocrit are not linear; even small increases above a certain threshold can significantly raise cardiovascular risk. The consensus among experts appears to be that levels over 54% are concerning.What are the general recommendations for managing high hematocrit on TRT?
Proper monitoring and management are essential. While the source does not detail specific management strategies, it emphasizes that elevated hematocrit is "not something to ignore." Other threads on the same forum, linked within the source, discuss methods like phlebotomy ("giving blood") as a common strategy to lower hematocrit. It also indirectly suggests that lifestyle factors like diet can play a role, although it's noted that some men on TRT might adopt worse diets despite increased gym activity.Key References
- Bachman E, Travison T G, Basaria S, et al. “Testosterone Induces Erythrocytosis via Increased Erythropoietin and Suppressed Hepcidin: Evidence for a New Erythropoietin/Hemoglobin Set Point.” J Gerontol A 2014;69(6):725-735.
Testosterone Induces Erythrocytosis via Increased Erythropoietin and Suppressed Hepcidin: Evidence for a New Erythropoietin/Hemoglobin Set Point - PMC pmc.ncbi.nlm.nih.gov - Coviello A D, Kaplan B, Lakshman K M, et al. “Effects of Graded Doses of Testosterone on Erythropoiesis in Healthy Young and Older Men.” J Clin Endocrinol Metab 2008;93(3):914-919.
Effects of graded doses of testosterone on erythropoiesis in healthy young and older men - PubMed pubmed.ncbi.nlm.nih.gov - Bhasin S, Brito J P, Cunningham G R, et al. “Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline.” J Clin Endocrinol Metab 2018;103(5):1715-1744.
Testosterone Therapy for Hypogonadism Guideline Resources endocrine.org - U.S. FDA. “Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging.” 2014.
FDA cautions about using testosterone products for low testosterone fda.gov - Kohn T P, Agrawal P, Ory J, et al. “Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy.” J Urol 2024;211(2):285-293.
Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy: A Retrospective Cohort Claims Database Analysis - PubMed pubmed.ncbi.nlm.nih.gov - Gagnon D R, Zhang T J, Brand F N, Kannel W B. “Hematocrit and the Risk of Cardiovascular Disease—The Framingham Study: 34-Year Follow-up.” Am Heart J 1994;127(3):674-682.
Hematocrit and the risk of cardiovascular disease--the Framingham study: a 34-year follow-up - PubMed pubmed.ncbi.nlm.nih.gov - Richalet J-P, Rivera M, Bouchet P, et al. “Acetazolamide: A Treatment for Chronic Mountain Sickness.” Am J Respir Crit Care Med 2005;172(11):1427-1433.
Acetazolamide: a treatment for chronic mountain sickness - PubMed pubmed.ncbi.nlm.nih.gov - Vásquez R, Villena M. “Normal Hematological Values for Healthy Persons Living at 4000 Meters in Bolivia.” High Alt Med Biol 2001;2(3):361-367.
Normal hematological values for healthy persons living at 4000 meters in Bolivia - PubMed pubmed.ncbi.nlm.nih.gov - Yin R, Wu Y, Li M, et al. “Association Between High-Altitude Polycythemia and Hypertension: A Cross-Sectional Study in Adults at Tibetan Ultrahigh Altitudes.” J Hum Hypertens 2024;38:555-560.
Association between high-altitude polycythemia and hypertension: a cross-sectional study in adults at Tibetan ultrahigh altitudes - Journal of Human Hypertension nature.com - Tang S, Zhou W, Chen L, et al. “High Altitude Polycythemia and Its Maladaptive Mechanisms: An Updated Review.” Front Med 2024;11:1448654.
Frontiers | High altitude polycythemia and its maladaptive mechanisms: an updated review frontiersin.org - Robinson N, Saugy M. “Altitude and Erythropoietin: Comparative Evaluation of Their Impact on Key Parameters of the Athlete Biological Passport—A Review.” Front Sports Act Living 2022;4:864532.
Frontiers | Altitude and Erythropoietin: Comparative Evaluation of Their Impact on Key Parameters of the Athlete Biological Passport: A Review frontiersin.org - Bigham A W, Beall C M. “High-Altitude Erythrocytosis: Mechanisms of Adaptive and Maladaptive Responses.” Physiology 2021;36:391-400.
https://journals.physiology.org/doi/10.1152/physiol.00029.2021 journals.physiology.org - Walker K M, Oprea C. “The Effect of Testosterone on Cardiovascular Disease and Thrombosis.” Curr Opin Cardiol 2021;36(6):767-774.
The Effect of Testosterone on Cardiovascular Disease and Cardiovascular Risk Factors in Men: A Review of Clinical and Preclinical Data - PubMed pubmed.ncbi.nlm.nih.gov - Basnyat B, Murdoch D R. “High-Altitude Illness.” BMJ 2019;368:l911.
High-altitude illness: Management approach - PMC pmc.ncbi.nlm.nih.gov - ExcelMale Forum Thread. “WARNING: Do not believe Internet ‘gurus’ proclaiming no need to manage hematocrit on TRT.” (Discussion thread, March 14 2025).
WARNING: Do not believe Internet "gurus" proclaiming no need to manage hematocrit on TRT - Excel Male TRT Forum
Last edited:




") .
.