diegoamartin7
New Member
Low SHBG issues dialing in,
So I started TRT again after taking a year off from it, pre try my leveled where 402 TT, 9FT, e2 24
had issues with libido , ED and morning wood nonexistant, plus some bad crash when i took proviron a couple times, felt horrendous like low T and low E2,
Tried clomid, gave me permanent eye floaters but i felt good on it, despite getting my test to just 710 and free test of 13, but ed and libido where not perfect
now I’m trying to do a simpler approach, enanthate only, sub q every day, 120mg a week
But there is a very poor reponse
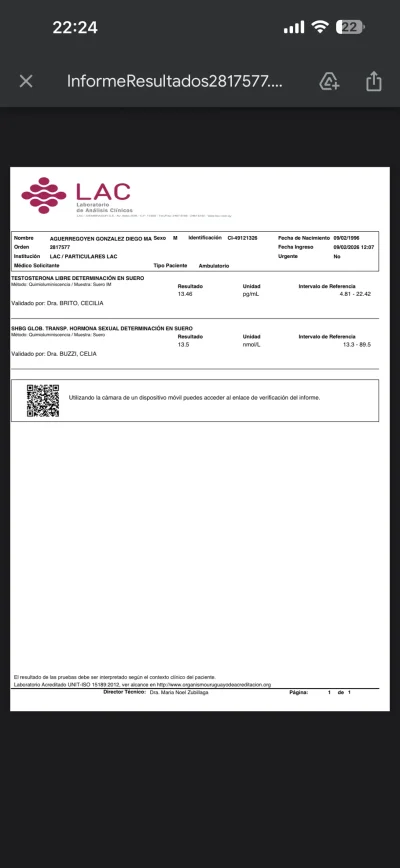
My shbg is low at 13.5
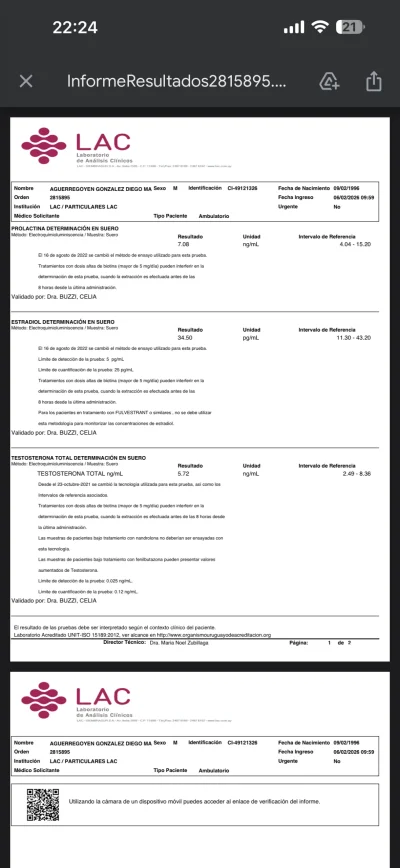
e2 mildly elevated at 34
prolactin at 7
totally test is 560
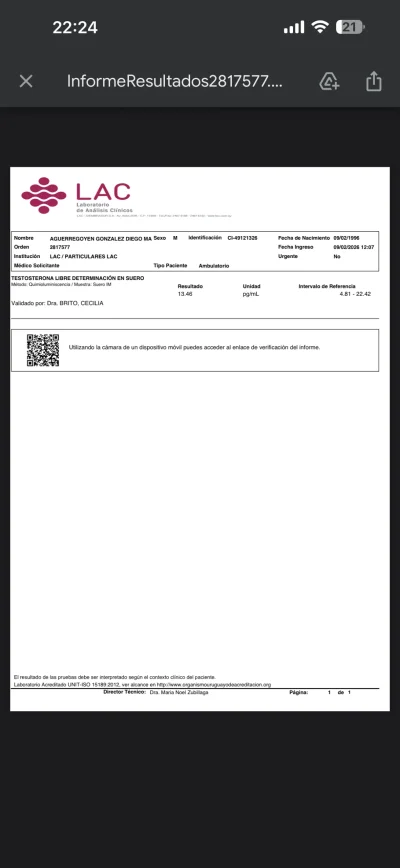
free test is 13,2
I’m having very bad ED issues, that are causing extreme depression, i’m feeling really bad guys, so bad i have considered suicide at times, because it’s so frustrating no being able to see the benefits of try and only making things worse.
My glycosilated hemoglobin is 4.8
tsh is at 2 (take 50mcg t4
Why proviron crashes me? why is my shbg is low and yet my free testosterone is also low? i feel like a ruined my life, any support would be appreciated
So I started TRT again after taking a year off from it, pre try my leveled where 402 TT, 9FT, e2 24
had issues with libido , ED and morning wood nonexistant, plus some bad crash when i took proviron a couple times, felt horrendous like low T and low E2,
Tried clomid, gave me permanent eye floaters but i felt good on it, despite getting my test to just 710 and free test of 13, but ed and libido where not perfect
now I’m trying to do a simpler approach, enanthate only, sub q every day, 120mg a week
But there is a very poor reponse
My shbg is low at 13.5
e2 mildly elevated at 34
prolactin at 7
totally test is 560
free test is 13,2
I’m having very bad ED issues, that are causing extreme depression, i’m feeling really bad guys, so bad i have considered suicide at times, because it’s so frustrating no being able to see the benefits of try and only making things worse.
My glycosilated hemoglobin is 4.8
tsh is at 2 (take 50mcg t4
Why proviron crashes me? why is my shbg is low and yet my free testosterone is also low? i feel like a ruined my life, any support would be appreciated