TestBoosted
Member
Hello friends,
Hope you are well!
I am a 33 year old male, height 183cm, weight 95kg with body fat around 20%.
Around 10 years ago, I was diagnosed with secondary hypogonadism. My natural T levels were 8 nMol/L and my FHS and LH were low. The main symptom that led me to do the blood test for testosterone was erectile dysfunction.
At the national hospital, they put me on tesosterone enanthate at 250mg every 3 weeks (1 shot every 3 weeks). Unfortunately, this didn't work for me. During the first week, I felt really anxious and panicky with headaches. During the second week, I used to feel so and so while on the 3rd week, I used to feel extremely tired and letarghic, with no energy. This continued for around a year and during that year my erections never improved.
After some time, I decided to try HCG monotherapy. Unfortunately, this used to spike my estrogen a lot and again I had to stop it. No improvements in erections.
Next, I tried Nebido. The first and second shot of 1000mg is given in 6 week intervals, with future shots being given in 10 week intervals. Along with CIalis 5mg, this gave me the best erections of my life. I used to wake up with very strong erections almost every day. Whenever I even had the slightest sexual thought of women or a woman touched me, I would get a strong erection instantly and sex was finally possible and enjoyable again. Past issues with premature ejactulation resolved as well and I was positive that I was finally cured.
Unfortunately, this only lasted around 2 years and my erectile dysfunction returned, even on the same protocol and trying to experiment with shortening or lengthening the injection intervals. Right now, I am only able to get soft erections only in specific positions, like when I am sitting on the toilet or manually stimulating. The head does not engorge and I lose the erections very quickly. PDE5 inhibitors like Viagra and Cialis no longer work, even if I try taking the maximum doses (100mg Viagra or 20 mg Cialis). The erections are not suitable for sexual intercourse as the head is very soft and the erection is lost quickly.
After a lot of reading on these forums, I decided to convince my doctor to go back to basics. No more Nebido, just get on testosterone enanthate and try frequent injections.
For the past 5 weeks, I have been taking testosterone enanthate, 2 injections per week on Monday evening and Friday morning (every 3.5 days). Each injection is 50 mg, for a total of 100 mg per week. I inject IM in the outer thigh.
I took bloods and you can find the results attached in this thread. These bloods were taken 5 weeks since starting the new protocol, on Friday morning just before next injection.
Some key takeaways:
i) Total testosterone is 19 nmol/L, which I believe is a good value for trough.
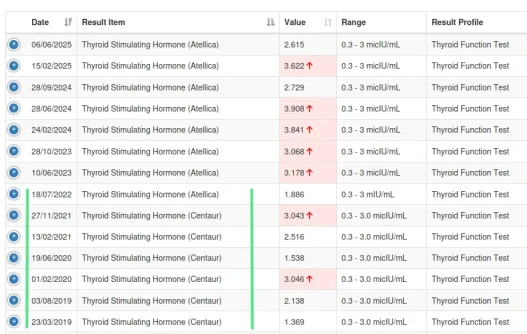
ii) Free thyroxine is very slightly elevated (20.64 pmol/L against a maximum of 20.3 pmol/L).
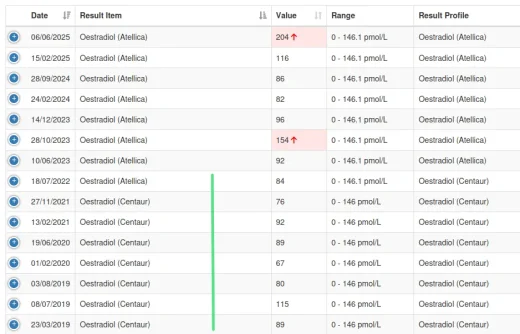
iii) Oestradiol seems to be very elevated and this is at trough level (204 pmol/L against a maximum of 146.1 pmol/L).
iv) Haemocrit is slightly elevated (51%)
Unfortunately, I tried getting SHBG tested but for some reason or another, they couldn't book it for me. I had tested for SHBG when I was originally on testosterone enanthate 250 mg every 3 weeks, and the value was around 18 to 21 around 6 years ago. In the future, I will try to test it privately along with total t and albumin so that I can then calculate free t.
I would like to get assistance on how to improve my TRT protocol for better erections. How can I improve it further please? Thank you so much for your dedication and assistance and apologies for the very long post.
EDIT
One last important piece of info.
I am currently taking these medications:
i) Anafranil (Antidepressant) - Lowest dose at 10mg
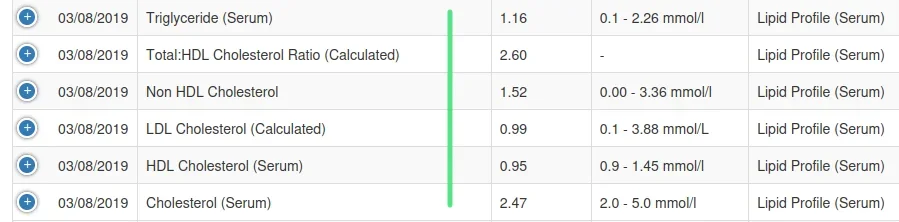
ii) Diagnosed with High cholesterol (Low HDL and high LDL) - Being controlled using Atorvastatin 20 mg
iii) Cialis 5 mg daily
Hope you are well!
I am a 33 year old male, height 183cm, weight 95kg with body fat around 20%.
Around 10 years ago, I was diagnosed with secondary hypogonadism. My natural T levels were 8 nMol/L and my FHS and LH were low. The main symptom that led me to do the blood test for testosterone was erectile dysfunction.
At the national hospital, they put me on tesosterone enanthate at 250mg every 3 weeks (1 shot every 3 weeks). Unfortunately, this didn't work for me. During the first week, I felt really anxious and panicky with headaches. During the second week, I used to feel so and so while on the 3rd week, I used to feel extremely tired and letarghic, with no energy. This continued for around a year and during that year my erections never improved.
After some time, I decided to try HCG monotherapy. Unfortunately, this used to spike my estrogen a lot and again I had to stop it. No improvements in erections.
Next, I tried Nebido. The first and second shot of 1000mg is given in 6 week intervals, with future shots being given in 10 week intervals. Along with CIalis 5mg, this gave me the best erections of my life. I used to wake up with very strong erections almost every day. Whenever I even had the slightest sexual thought of women or a woman touched me, I would get a strong erection instantly and sex was finally possible and enjoyable again. Past issues with premature ejactulation resolved as well and I was positive that I was finally cured.
Unfortunately, this only lasted around 2 years and my erectile dysfunction returned, even on the same protocol and trying to experiment with shortening or lengthening the injection intervals. Right now, I am only able to get soft erections only in specific positions, like when I am sitting on the toilet or manually stimulating. The head does not engorge and I lose the erections very quickly. PDE5 inhibitors like Viagra and Cialis no longer work, even if I try taking the maximum doses (100mg Viagra or 20 mg Cialis). The erections are not suitable for sexual intercourse as the head is very soft and the erection is lost quickly.
After a lot of reading on these forums, I decided to convince my doctor to go back to basics. No more Nebido, just get on testosterone enanthate and try frequent injections.
For the past 5 weeks, I have been taking testosterone enanthate, 2 injections per week on Monday evening and Friday morning (every 3.5 days). Each injection is 50 mg, for a total of 100 mg per week. I inject IM in the outer thigh.
I took bloods and you can find the results attached in this thread. These bloods were taken 5 weeks since starting the new protocol, on Friday morning just before next injection.
Some key takeaways:
i) Total testosterone is 19 nmol/L, which I believe is a good value for trough.
ii) Free thyroxine is very slightly elevated (20.64 pmol/L against a maximum of 20.3 pmol/L).
iii) Oestradiol seems to be very elevated and this is at trough level (204 pmol/L against a maximum of 146.1 pmol/L).
iv) Haemocrit is slightly elevated (51%)
Unfortunately, I tried getting SHBG tested but for some reason or another, they couldn't book it for me. I had tested for SHBG when I was originally on testosterone enanthate 250 mg every 3 weeks, and the value was around 18 to 21 around 6 years ago. In the future, I will try to test it privately along with total t and albumin so that I can then calculate free t.
I would like to get assistance on how to improve my TRT protocol for better erections. How can I improve it further please? Thank you so much for your dedication and assistance and apologies for the very long post.
EDIT
One last important piece of info.
I am currently taking these medications:
i) Anafranil (Antidepressant) - Lowest dose at 10mg
ii) Diagnosed with High cholesterol (Low HDL and high LDL) - Being controlled using Atorvastatin 20 mg
iii) Cialis 5 mg daily