Despite the highly theoretical nature of your position, I would be inclined to agree that there would be a dosage of exogenous testosterone that, after long periods of exposure would bring about some toxic effects to the body; neural apoptosis is currently cited in the literature. However, the continuous circle we go around in this forum is what is that dosage?A key degree of freedom (that makes your question difficult to answer with a reasonable degree of confidence) is time.
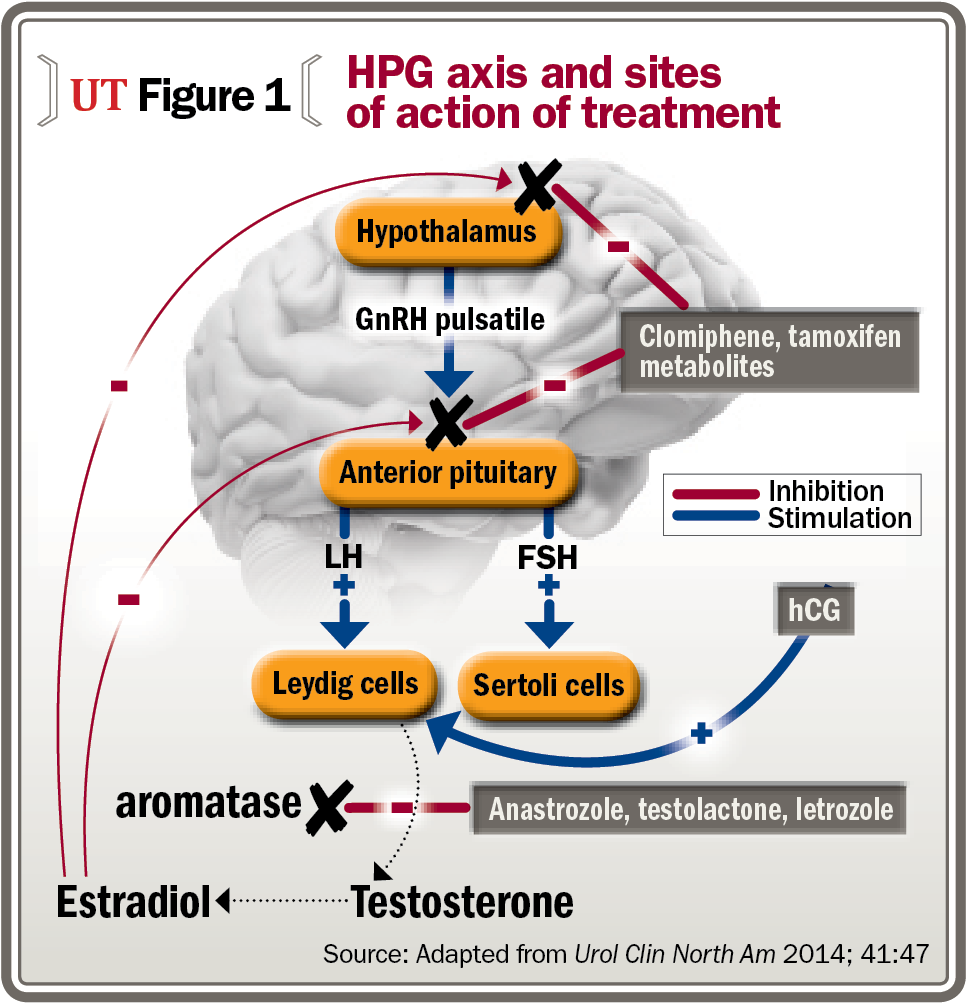
Chronic toxicity or acute toxicity? The figure above, while simplified, is instructive as an introduction. Add time above to make a 3d plot which would consider chronic toxicity.
Most studies I've reviewed and anecdotal / empirical data suggests little to minor acute toxicity with injectable non-17aa AAS (studies exploring injectable AAS - including T - for 4 to 10 weeks).
Regarding chronic toxicity, which is the integral of acute toxicity over time, I'd propose the following;
CT = Integral [f(d, g, Ho, A) dt] | limits of integration from time zero (start use) to endpoint
where
CT is chronic toxicity
d is instantaneous dose
g is genome of an individual
Ho is health markers or "health" at time zero
A is age at time zero
A reasonable mechanistic picture of chronic toxicity (e.g., heart) from supraphysiologic testosterone use can be deduced from the current body of scientific literature as well as anecdotal data points. The old rule of thumb of time on = time off applies to Test cycles just like other AAS cycles. If it didn't we would all be running 1 g of test per week continuously with no consequences (wouldn't that be nice?).
Or if it is simpler, a decent analogy can be made between recreational AAS abuse and cigarettes. Long term the story for a significant fraction of abusers does not end well. At the individual level, what's the outcome of running 1100 or 1500 ng/dl TT for 1 year, 5 years, 10 years continuously? I have no idea. One way to find out.
Report back after a few years. I shared my experience; I sincerely hope you have a better experience. Make sure you make the decision with informed consent.
There’s been a prevailing thought among a few influential members of this forum that posit the toxic number to be anything greater than the currently accepted statistical mean testosterone levels.
Though not explicitly stated, advice given to many new members on this forum is to lower exogenous testosterone dosage down to a level that produces TT near the statistical average, and all/most all side effects will resolve.
Tell me @readalot, what body of literature or strong anecdotal evidence are you referring to when you position your argument that a total testosterone of ~1200 ng/dL is reaching a toxic level?