

High hematocrit, low ferritin and thyroid.
Does taking 15 mg of ferrous sulfate increase ferritin?
Hello everybody. I will attach my exams below and I would like your opinion. Thank you very much.
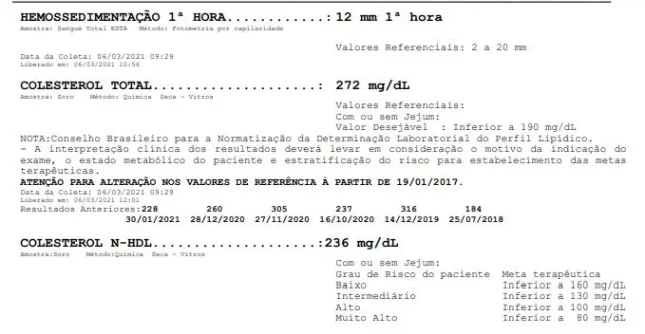
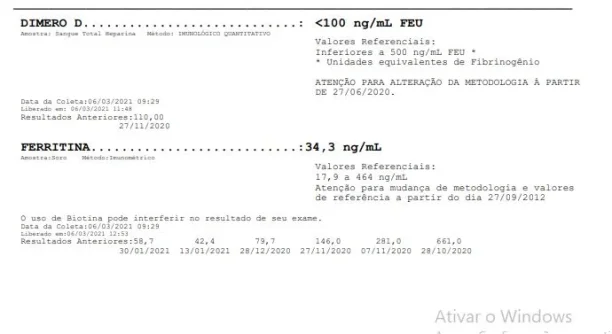
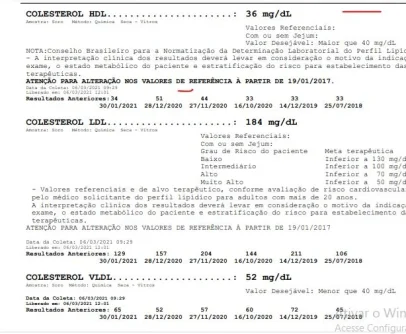
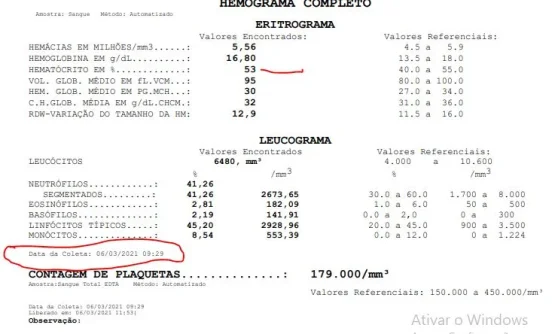
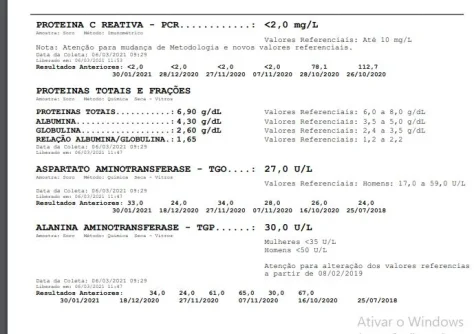
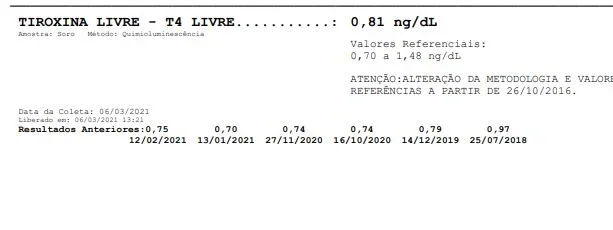
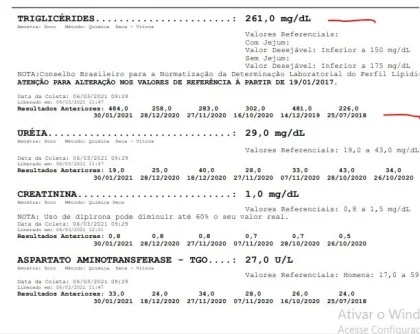
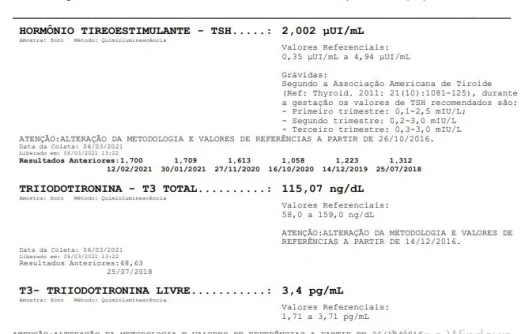
In early January of this year I had a phlebotomy due to an increase in hematocrit. I only did this once. My triglycerides and cholesterol are always high and I have to be very attentive to my diet. My thyroid needs to be optimized and when I did that the serum iron and ferritin levels went down but the hematocrit is very high.
Some days I have woken up very weak and the desire is to continue to lie down. 30 days ago I started supplementing 25 mcg T4 + 1 mcg T3. I also take 2 drops of lugol in the morning + 200 mcg of chelated selenium + 30 mg of zinc to try to improve the thyroid. Is it because of this supplementation that my ferritin has decreased since the thyroid consumes a lot of iron? And the problem is the hematocrit that is high 53 and at this level I cannot do a phlebotomy and if supplemented with iron, that hematocrit tends to get higher. I had a covid in October 2020. Will it be a sequel to the covid and my blood oxygen is low and the hematocrit increases because of that? Will I have to stop Trt to try to stabilize all of this?
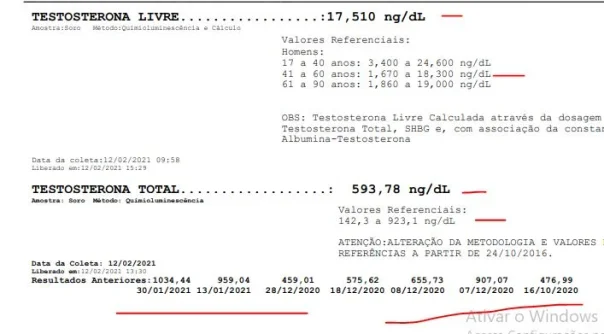
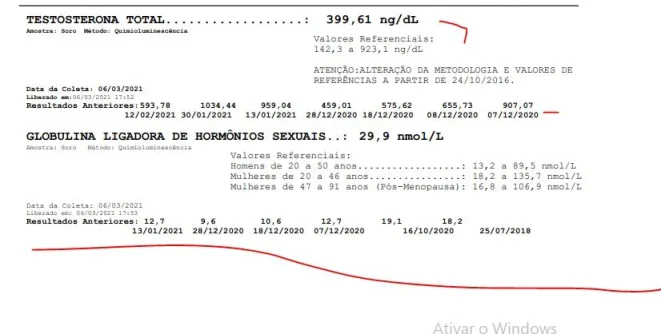
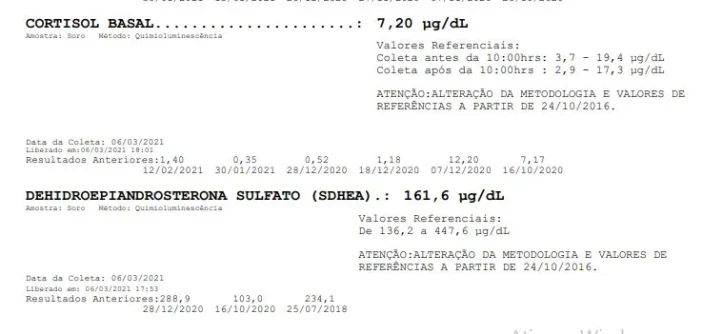
I have been lowering Trt doses due to hematocrit and side effects that increase my blood pressure. I am currently injecting 15 Mg E3D enanthate + 250 ui Hcg twice a week + 24 Mg Dhea ED. Low shbg. 12.7.
Does taking 15 mg of ferrous sulfate increase ferritin?
Hello everybody. I will attach my exams below and I would like your opinion. Thank you very much.
In early January of this year I had a phlebotomy due to an increase in hematocrit. I only did this once. My triglycerides and cholesterol are always high and I have to be very attentive to my diet. My thyroid needs to be optimized and when I did that the serum iron and ferritin levels went down but the hematocrit is very high.
Some days I have woken up very weak and the desire is to continue to lie down. 30 days ago I started supplementing 25 mcg T4 + 1 mcg T3. I also take 2 drops of lugol in the morning + 200 mcg of chelated selenium + 30 mg of zinc to try to improve the thyroid. Is it because of this supplementation that my ferritin has decreased since the thyroid consumes a lot of iron? And the problem is the hematocrit that is high 53 and at this level I cannot do a phlebotomy and if supplemented with iron, that hematocrit tends to get higher. I had a covid in October 2020. Will it be a sequel to the covid and my blood oxygen is low and the hematocrit increases because of that? Will I have to stop Trt to try to stabilize all of this?
I have been lowering Trt doses due to hematocrit and side effects that increase my blood pressure. I am currently injecting 15 Mg E3D enanthate + 250 ui Hcg twice a week + 24 Mg Dhea ED. Low shbg. 12.7.
Attachments
-
 colesterol.webp37.2 KB · Views: 222
colesterol.webp37.2 KB · Views: 222 -
 ferritina06-03-2021.webp23.2 KB · Views: 238
ferritina06-03-2021.webp23.2 KB · Views: 238 -
 ferroserico06-03-2021.webp50.6 KB · Views: 209
ferroserico06-03-2021.webp50.6 KB · Views: 209 -
 glicemia.webp21 KB · Views: 220
glicemia.webp21 KB · Views: 220 -
 hdl.webp59.3 KB · Views: 212
hdl.webp59.3 KB · Views: 212 -
 hemograma06-03-2021.webp43.1 KB · Views: 218
hemograma06-03-2021.webp43.1 KB · Views: 218 -
 proteinacreativa.webp47.7 KB · Views: 218
proteinacreativa.webp47.7 KB · Views: 218 -
 t3reverso.webp36 KB · Views: 214
t3reverso.webp36 KB · Views: 214 -
 t4.webp12.3 KB · Views: 199
t4.webp12.3 KB · Views: 199 -
 testosterona.webp33.3 KB · Views: 216
testosterona.webp33.3 KB · Views: 216

.png")










