Spartan1985
Member
Hi guys
Further to the great support received previously I was hoping some of you would be able to look at the results from my recent bloods and offer some feedback.
Overview- had numerous issues since starting TRT with little to no benefit. Following the great advice of some members I dropped dose to 10mg prop subQ daily which gave me the best results yet. Libido returned although still quite reserved. Some improvement in erection quality and training recovery.
Was training hard for a holiday (vanity quest) and hit major burnout so in a moment of weakness decided a 12 week one rip (test p, mast, tren mix) was worth doing at 1.5ml 3 times a week. Had a great 8 weeks of sex drive, better erections and recovery then last 4 as usual for me were a gradual decline.
Off for around a month now, week of tamoxifen and hcg then back to 10mg prop a day subQ.
Feeling pretty shit at the moment, little to no penile sensitivity, poor erection quality, struggle to ejaculate, overall kinda dry feeling down there.
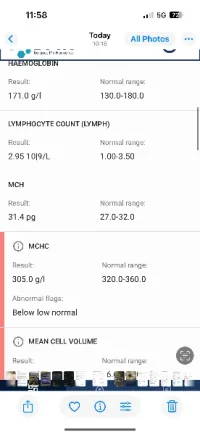
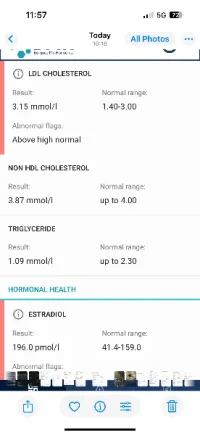
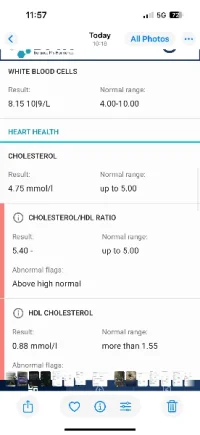
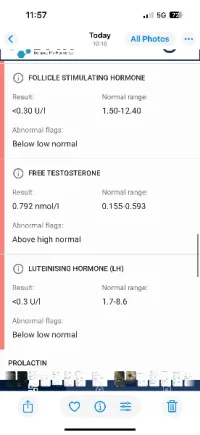
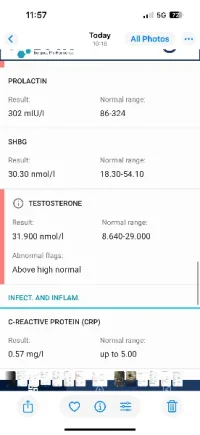
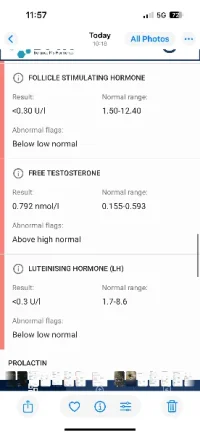
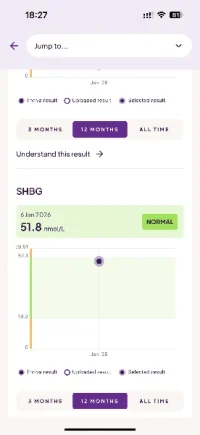
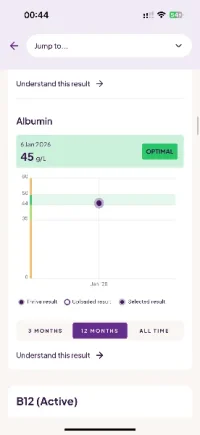
Had bloods done and attached the results. Loads of markers outwith normal range.
As ED has been an increasing issue even prior to the last cycle does anyone see any contributing factors in these results?
Oestrogen seems high, don’t cope well with AI seems to floor it almost straight away and leads to more side effects is there any better way to manage this?
How do you guys see the test range (slightly above normal for both T and free T? Protocol seem ok or should I adjust dose?
Any feedback greatly appreciated as these numbers mean very little to me
Further to the great support received previously I was hoping some of you would be able to look at the results from my recent bloods and offer some feedback.
Overview- had numerous issues since starting TRT with little to no benefit. Following the great advice of some members I dropped dose to 10mg prop subQ daily which gave me the best results yet. Libido returned although still quite reserved. Some improvement in erection quality and training recovery.
Was training hard for a holiday (vanity quest) and hit major burnout so in a moment of weakness decided a 12 week one rip (test p, mast, tren mix) was worth doing at 1.5ml 3 times a week. Had a great 8 weeks of sex drive, better erections and recovery then last 4 as usual for me were a gradual decline.
Off for around a month now, week of tamoxifen and hcg then back to 10mg prop a day subQ.
Feeling pretty shit at the moment, little to no penile sensitivity, poor erection quality, struggle to ejaculate, overall kinda dry feeling down there.
Had bloods done and attached the results. Loads of markers outwith normal range.
As ED has been an increasing issue even prior to the last cycle does anyone see any contributing factors in these results?
Oestrogen seems high, don’t cope well with AI seems to floor it almost straight away and leads to more side effects is there any better way to manage this?
How do you guys see the test range (slightly above normal for both T and free T? Protocol seem ok or should I adjust dose?
Any feedback greatly appreciated as these numbers mean very little to me