Welcome to
ExcelMale. I am glad you joined us.
I am glad that you got diagnosed and that you are post-op. Now it's time to rebuild your hormones!
I did a deep dive on your condition and came up with a few suggestions.
Does hypogonadism resolve after surgery removal of A-Craniopharyngioma?
Short answer: No, hypogonadism rarely resolves after craniopharyngioma surgery—and it frequently worsens.
The evidence is quite consistent on this point:
Pre- vs Post-operative Hypogonadism Rates
The preoperative hypogonadism incidence in craniopharyngioma patients was 74.2%, which increased to 90.9% postoperatively.
PubMed Central Preservation of the pituitary stalk does not lead to restoration of the pituitary-gonadal axis in 83% of cases.
Endocrine Abstracts
Why Recovery Is Exceptional
The recovery of any deficient adenohypophysial hormone in the preoperative study, sometimes occurring after surgery for a pituitary macroadenoma, is exceptional in patients with craniopharyngioma.
Elsevier This contrasts sharply with pituitary adenomas, where about half of preoperative deficiencies can recover.
No patients with a craniopharyngioma or meningioma had resolution of hypopituitarism after transsphenoidal surgery, while new hypopituitarism occurred in approximately one third of patients.
PubMed
Overall Pituitary Dysfunction Post-Surgery
The proportion of patients with deficiency of some adenohypophysial hormone reaches 87–95% after tumor surgery, regardless of whether a transsphenoidal or transcranial approach is used or whether total or partial tumor resection is performed.
Elsevier
Clinical Implications
Patients should expect
lifelong testosterone replacement therapy post-craniopharyngioma resection. Due to the high prevalence of post-operative hypothalamic-pituitary dysfunction, patients with craniopharyngioma usually require long-term multiple hormone substitution therapy.
PubMed Central
The best-case scenario from one surgical series showed gonadal function was the axis
least likely to worsen—but that's only relative to other axes, not actual recovery.
Suggestion: Start testosterone cypionate or enanthate injections at 75 mg twice per week plus hCG 500 IU twice per week. Watch this video on how I do it:
Nelson Vergel 's Testosterone plus HCG Protocol - Excel Male Health Forum
Also, have your doctor perform blood tests as listed below to find out if you are also deficient in other hormones. You can choose to do this 6 weeks after doing the TRT+hCG protocol.
3-MONTH POST-OP ASSESSMENT
This is a critical evaluation point. All axes should be tested to establish post-surgical baseline and guide hormone replacement.
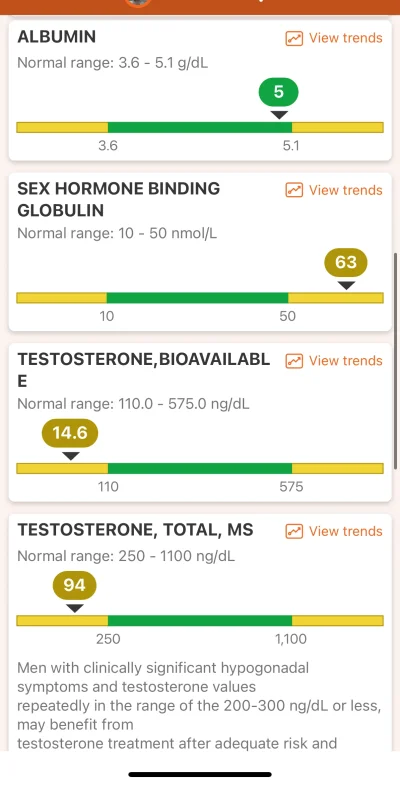
Gonadal Axis (Secondary Hypogonadism)
| ✓ | Test | Result | Range | Date |
☐ | Total Testosterone | | | |
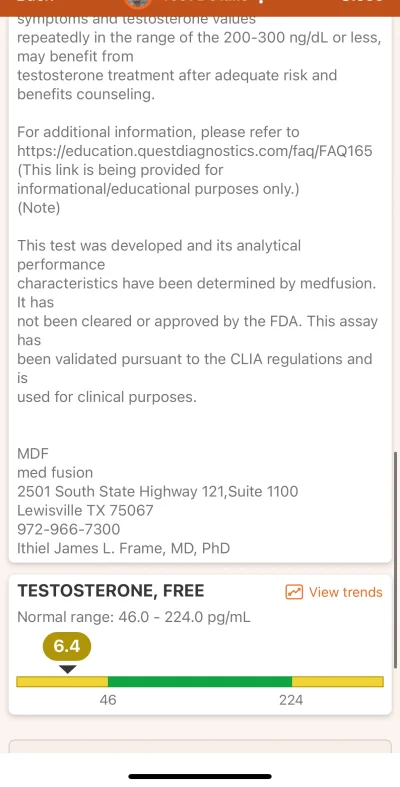
☐ | Free Testosterone | | | |
☐ | LH | | | |
☐ | FSH | | | |
☐ | SHBG | | | |
☐ | Estradiol (E2) | | | |
Note: Low/normal LH and FSH with low testosterone confirms secondary (central) hypogonadism. Morning draw essential.
Thyroid Axis (Central Hypothyroidism)
| ✓ | Test | Result | Range | Date |
☐ | Free T4 | | | |
☐ | Free T3 | | | |
☐ | TSH | | | |
Critical: TSH is unreliable in central hypothyroidism. Dose adjustments should target Free T4 in mid-to-upper normal range.
Adrenal Axis (Secondary Adrenal Insufficiency)
| ✓ | Test | Result | Range | Date |
☐ | Morning Cortisol (8am, before HC dose) | | | |
☐ | ACTH | | | |
If on hydrocortisone: draw morning cortisol BEFORE taking AM dose. Clinical symptoms guide dosing more than labs.
Growth Hormone Axis
| ✓ | Test | Result | Range | Date |
☐ | IGF-1 | | | |
GH deficiency is very common post-craniopharyngioma. Low IGF-1 supports diagnosis; stimulation testing may be needed.
Prolactin & Water Balance
| ✓ | Test | Result | Range | Date |
☐ | Prolactin | | | |
☐ | Serum Sodium | | | |
☐ | Serum Osmolality | | | |
Monitor sodium if on DDAVP. Hyponatremia indicates overtreatment; hypernatremia indicates undertreatment.
Metabolic Health (Baseline & Monitoring)
| ✓ | Test | Result | Range | Date |
☐ | Fasting Glucose | | | |
☐ | HbA1c | | | |
☐ | Fasting Lipid Panel | | | |
☐ | Comprehensive Metabolic Panel | | | |
☐ | CBC | | | |
☐ | Vitamin D, 25-OH | | | |
Hypothalamic obesity and metabolic syndrome are common after craniopharyngioma. Monitor closely.
TRT MONITORING (8 Weeks on Testosterone)
These tests monitor safety and optimization of testosterone replacement therapy.
✓ |
Test |
Result |
Range |
Date |
☐ | Hematocrit / Hemoglobin | | | |
☐ | Prolactin & IGF-1 | | | |
☐ | Estradiol (E2) Sensitive | | | |
☐ | Total Testosterone (trough) | | | |
☐ | Free Testosterone Eq. Dialysis | | | |
Draw trough levels (day before next injection for weekly protocols, or morning for daily gels/creams).
LONG-TERM MONITORING SCHEDULE
Timeframe |
Tests Required |
Every 3-6 months |
Complete pituitary panel, metabolic labs, TRT monitoring if applicable |
Every 6-12 months |
MRI surveillance for tumor recurrence, IGF-1, comprehensive metabolic assessment |
Annually |
Full endocrine evaluation, lipid panel, HbA1c, bone density (DEXA) if GH deficient |