Hi Team - 5 weeks in 200mg Test 1x weekly due to total T being at 319 most of my life (I’m now 49). I’m 6’1, 221 lbs and after 5 weeks, weight same, but gained 4 lbs of muscle, lost 4 lbs of fat. My clinic uses Inbody scan and it shows my percent body fat going from 26 to 22.6.
I have felt TONS of energy, high libido, and starting to see physical change. However, I have also had horrible insomnia. And…as of last 2 days, I’m starting to lose morning erections. Due to insomnia, I did reduce my last shot from 200 to 150. The last shot was 3 days ago.
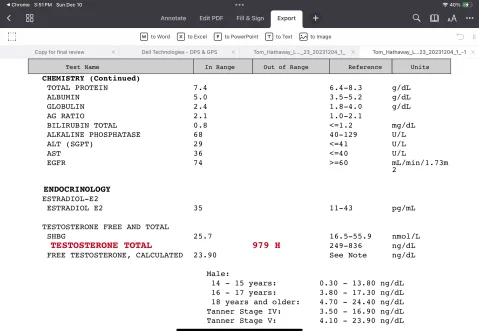
Had blood drawn past week and will have results in a few days, but here are my questions.
-should I reduce my Test to 100, or 150?
-clinic prescribed me Anastrozle and Enclomiphene, but told me to hold off taking until first flood draw. Should I start low doses of these?
-does my symptoms of insomnia and now lowered sex drive indicate Estrogen issue?
-Also, I just ordered 90 day supply of Semorelin…objective is more muscle! Will this interfere with my TRT/Estrogen balance? Should I consider holding off on this until I get the right balance?
Thanks
Welcome to Nelson's domain!
Hi Team - 5 weeks in 200mg Test 1x weekly due to total T being at 319 most of my life (I’m now 49)
This is a myth that needs to be put to rest.
Even if your TT was lower it does not mean you would need a high dose of androgens to achieve a healthy let alone high trough FT level.
The common starting dose across the board is 100 mg T/week.
Most men are injecting 100-200 mg T/week strictly IM (shallow/deep) or subcutaneously whether once weekly, or split into twice-weekly (every 3.5 days), M/W/F, EOD, or daily.
Even then a majority of men would never need the high-end dose 200 mg T/week to achieve a healthy let alone high trough FT level.
Are there what we call those outliers, most definitely but it is FAR from COMMON.
Most men can easily achieve a healthy/high or in some cases very high trough FT injecting 100-150mg T/week especially when split into more frequent injections.
Unfortunately, you were overmedicated from the get-go.
Piss poor protocol starting a man out on 200 mg T/week.
The best piece of advice is to start low and go slow on a T-only protocol.
Ancillaries such as hCG can eventually be added if need be.
Would try to avoid using an AI!
I have felt TONS of energy, high libido, and starting to see physical change. However, I have also had horrible insomnia. And…as of last 2 days, I’m starting to lose morning erections
This would be what we call the honeymoon period where one tends to experience a euphoric-like feeling, increased energy, and an increase in libido/erections when first starting due to rising T levels, and increased dopamine/lighting up of the AR.
Unfortunately for many, this is temporary and short-lived as the body will eventually adapt to the new set-point and things will level off more into what we call the norm.
Good chance your TT, FT, and estradiol levels are going to be very high on such a dose let alone it is a given that you are going to drive up other critical blood markers such as RBCs, hemoglobin, and hematocrit.
Hard to pinpoint what may be the cause of your erectile issues as we are shooting in the dark here without a full set of labs.
Keep in mind that testosterone has a tonic effect on the CNS and can easily make one feel amped up/on edge which can have a negative impact on sleep.
Chances are your TT and more importantly FT level is sky-high on such a dose!
Had blood drawn past week and will have results in a few days, but here are my questions.
-should I reduce my Test to 100, or 150?
-clinic prescribed me Anastrozle and Enclomiphene, but told me to hold off taking until first flood draw. Should I start low doses of these?
-does my symptoms of insomnia and now lowered sex drive indicate Estrogen issue?
Would be a wise move to decrease your dose as you were jacked up on T from the get-go.
100 or 120 mg T once weekly or better yet split into twice-weekly injections would be a good starting point.
Lots of time to increase the dose down the road if need be!
Drop the AI and the addition of
enclomiphene is a waste of time as your hpta will be shut down when using exogenous T.
Again we need a full set of labs before jumping to any conclusions.
Libido let alone ED are multifactorial.