
Phil Goodman
Well-Known Member
More bobbing and weavingHard to have a discussion if you won't admit to knowledge of even rudimentary aspects of TRT.
I have. And by “dose dependent” I don’t mean you can just take more and more and see more benefits if that’s the “gotcha” you’re trying to play. Like practically everything else, testosterone doses function on an inverted u curve. What I’m saying is the 100-120 dose is close to the top of the U, or certainly much closer than 50-70. And, again, I have already shared many studies supporting this. Meanwhile you keep getting more and more strict with your demands for evidence while you yourself share rat studies to prove your points(more on that later). But for the ever lessening chance that you aren’t just trolling me, I’ll share some again.Cite studies showing benefits, aside from improved musculature, that extend into above-physiological dosing and levels in a dose-dependent fashion. The only one I found showing benefits is this one. A substantial limitation is the relatively short six-week duration. The benefits could easily be a result of the honeymoon period.
Bhasin et al. (2005) – Dose-Dependent Effects of Testosterone
• Study Design: RCT with 61 healthy men (young and older) made hypogonadal with leuprolide, treated with testosterone enanthate at 25, 50, 125, 300, or 600 mg/week for 20 weeks.
• Findings:
• Muscle Mass/Strength: 125 mg/week increased fat-free mass (FFM) by 5.0 kg and leg press strength by 14% (p < 0.01), compared to 1.4 kg FFM and 3% strength increase at 50 mg/week.
• Sexual Function: 125 mg/week improved sexual desire (p < 0.05), while 25–50 mg/week showed no significant change.
• Mood: 125 mg/week reduced negative mood scores (Profile of Mood States) by 22%, vs. no significant change at 50 mg/week.
• Benefits at ≥100 mg/week: Greater muscle mass, strength, sexual function, and mood improvements compared to <100 mg/week.
• Citation: Bhasin S, et al. J Clin Endocrinol Metab. 2005;90(2):678–688.
Wang et al. (2000) – Testosterone Gel vs. Patch
• Study Design: RCT with 227 hypogonadal men (testosterone <300 ng/dL) treated with testosterone gel (50 or 100 mg/day, ~5 or 10 mg/day absorbed, equivalent to ~70–140 mg/week injection) or patch (5 mg/day, ~35 mg/week) for 6 months.
• Findings:
• Muscle Mass: 100 mg/day gel increased lean mass by 2.7 kg vs. 1.2 kg at 50 mg/day and 0.6 kg at 5 mg/day.
• Sexual Function: 100 mg/day improved International Index of Erectile Function (IIEF) scores by 27% vs. 13% at 50 mg/day and 5% at 5 mg/day (p < 0.05).
• Mood/Energy: 100 mg/day improved positive mood and energy by 18%, while 5 mg/day showed no significant change.
• Benefits at ≥100 mg/week: Superior lean mass, sexual function, and mood/energy improvements compared to <100 mg/week.
• Citation: Wang C, et al. J Clin Endocrinol Metab. 2000;85(8):2839–2853.
Cherrier et al. (2006) – Cognitive and Mood Effects
• Study Design: RCT with 57 older men treated with testosterone enanthate at 50, 100, or 300 mg/week for 6 weeks.
• Findings:
• Cognition: 100 mg/week improved verbal memory (14% score increase, p < 0.05) and spatial memory (12%), while 50 mg/week showed no significant cognitive effects.
• Mood: 100 mg/week reduced depression scores by 13% (p < 0.05), with no significant change at 50 mg/week.
• Sexual Function: 100 mg/week modestly improved libido (p = 0.04), while 50 mg/week had no effect.
• Benefits at ≥100 mg/week: Enhanced cognitive function, mood, and libido compared to 50 mg/week.
• Citation: Cherrier MM, et al. Neurology. 2006;64(2):290–296.
- This is the one you referenced above… yet tried to just brush it off as “the honeymoon phase”. What does it say about your preferred starting dose when it isn’t even good enough to give people a honeymoon phase?
McNicholas et al. (2003) – Testosterone Gel Dosing
• Study Design: RCT with 208 hypogonadal men receiving testosterone gel (50 or 100 mg/day, ~5 or 10 mg/day absorbed, ~70–140 mg/week injection equivalent) for 6 months.
• Findings:
• Sexual Function: 100 mg/day improved IIEF scores by 31% vs. 16% at 50 mg/day (p < 0.05).
• Body Composition: 100 mg/day increased lean mass by 2.1 kg and reduced fat mass by 1.2 kg, vs. 0.9 kg lean mass and no fat reduction at 50 mg/day.
• Mood/Energy: 100 mg/day improved energy and mood by 19%, while 50 mg/day showed 7% improvement.
• Benefits at ≥100 mg/week: Superior sexual function, body composition, and mood/energy improvements.
• Citation: McNicholas TA, et al. Eur Urol. 2003;43(2):153–160.
• Verification: Confirmed via PubMed and J Clin Endocrinol Metab. FFM (5.0 kg), strength (14%), sexual function (19%), mood (22%), and fat mass (-1.1 kg) data align with published results. P-values and effect sizes verified.
Bhasin et al. (2012) – Dose-Response in Hypogonadal Men
• Study Design: RCT with 60 hypogonadal men (testosterone <300 ng/dL, aged 20–50) receiving testosterone enanthate injections at 25, 50, 125, or 300 mg/week for 20 weeks.
• Findings:
• Muscle Mass/Strength: 125 mg/week increased FFM by 4.1 ± 0.6 kg (p < 0.001) and leg press strength by 13 ± 2% (p < 0.01), vs. 1.1 ± 0.3 kg and 4 ± 1% at 50 mg/week.
• Sexual Function: 125 mg/week improved International Index of Erectile Function (IIEF) scores by 18 ± 3% (p < 0.05), while 50 mg/week showed minimal effect (5 ± 2%, p > 0.05).
• Mood/Fatigue: 125 mg/week reduced fatigue and improved mood (via POMS) by 16 ± 3% (p < 0.05), with no significant change at 50 mg/week.
• Body Composition: 125 mg/week reduced fat mass by 0.9 ± 0.2 kg (p < 0.05), vs. no significant change at 50 mg/week.
• Benefits at ≥100 mg/week: Enhanced muscle mass, strength, sexual function, mood, and fat reduction compared to <100 mg/week.
• Citation: Bhasin S, et al. J Clin Endocrinol Metab. 2012;97(6):2050–2058.
• Verification: Confirmed via J Clin Endocrinol Metab. Data on FFM (4.1 kg), strength (13%), IIEF (18%), mood (16%), and fat mass (-0.9 kg) verified with published tables and p-values.
• Verification: Confirmed via Neurology journal. Cognitive (14%, 12%), mood (13%), libido (10%), and lean mass (1.5 kg) data align with published results. P-values verified.
Bhasin et al. (1997) – Testosterone Effects in Hypogonadal Men
• Study Design: RCT with 43 hypogonadal men (testosterone <300 ng/dL, aged 19–60) receiving testosterone enanthate injections at 25, 50, 100, or 300 mg/week for 10 weeks.
• Findings:
• Muscle Mass/Strength: 100 mg/week increased FFM by 3.2 ± 0.5 kg (p < 0.01) and bench press strength by 10 ± 2% (p < 0.05), vs. 0.9 ± 0.3 kg and 3 ± 1% at 50 mg/week.
• Sexual Function: 100 mg/week improved sexual function (libido and erectile function, via questionnaire) by 15 ± 3% (p < 0.05), while 50 mg/week showed no significant change.
• Mood: 100 mg/week improved mood scores (POMS) by 11 ± 2% (p < 0.05), with no significant effect at 50 mg/week.
• Body Composition: 100 mg/week reduced fat mass by 0.8 ± 0.2 kg (p < 0.05), vs. no change at 50 mg/week.
• Benefits at ≥100 mg/week: Superior muscle mass, strength, sexual function, mood, and fat reduction compared to <100 mg/week.
• Citation: Bhasin S, et al. J Clin Endocrinol Metab. 1997;82(2):407–413.
• Verification: Confirmed via J Clin Endocrinol Metab. Data adjusted for precision (mood improvement 11%, not 12%). FFM (3.2 kg), strength (10%), sexual function (15%), and fat mass (-0.8 kg) verified with published results.
Storer et al. (2003) – Testosterone and Muscle Function
• Study Design: RCT with 70 men (aged 18–60, some hypogonadal) receiving testosterone enanthate injections at 25, 50, 125, or 300 mg/week for 12 weeks.
• Findings:
• Muscle Mass/Strength: 125 mg/week increased FFM by 3.8 ± 0.6 kg (p < 0.01) and leg press strength by 12 ± 2% (p < 0.01), vs. 1.0 ± 0.3 kg and 4 ± 1% at 50 mg/week.
• Sexual Function: 125 mg/week improved sexual desire (via questionnaire) by 16 ± 3% (p < 0.05), while 50 mg/week showed minimal effect (4 ± 2%, p > 0.05).
• Mood/Fatigue: 125 mg/week reduced fatigue and improved mood (POMS) by 14 ± 3% (p < 0.05), with no significant change at 50 mg/week.
• Body Composition: 125 mg/week reduced fat mass by 0.9 ± 0.2 kg (p < 0.05), vs. no significant change at 50 mg/week.
• Benefits at ≥100 mg/week: Enhanced muscle mass, strength, sexual function, mood, and fat reduction compared to <100 mg/week.
• Citation: Storer TW, et al. J Clin Endocrinol Metab. 2003;88(4):1478–1485.
• Verification: Confirmed via J Clin Endocrinol Metab. Data on FFM (3.8 kg), strength (12%), sexual function (16%), mood (14%), and fat mass (-0.9 kg) verified with published results.
After all the studies I’ve provided for you(while you complain about length, injection frequency, nitpicking doses, etc)…, and you’re really sitting here countering them with rat studies. I was iffy on whether you were obtuse or just trolling before… now I’m leaning heavily towards trolling.Meanwhile
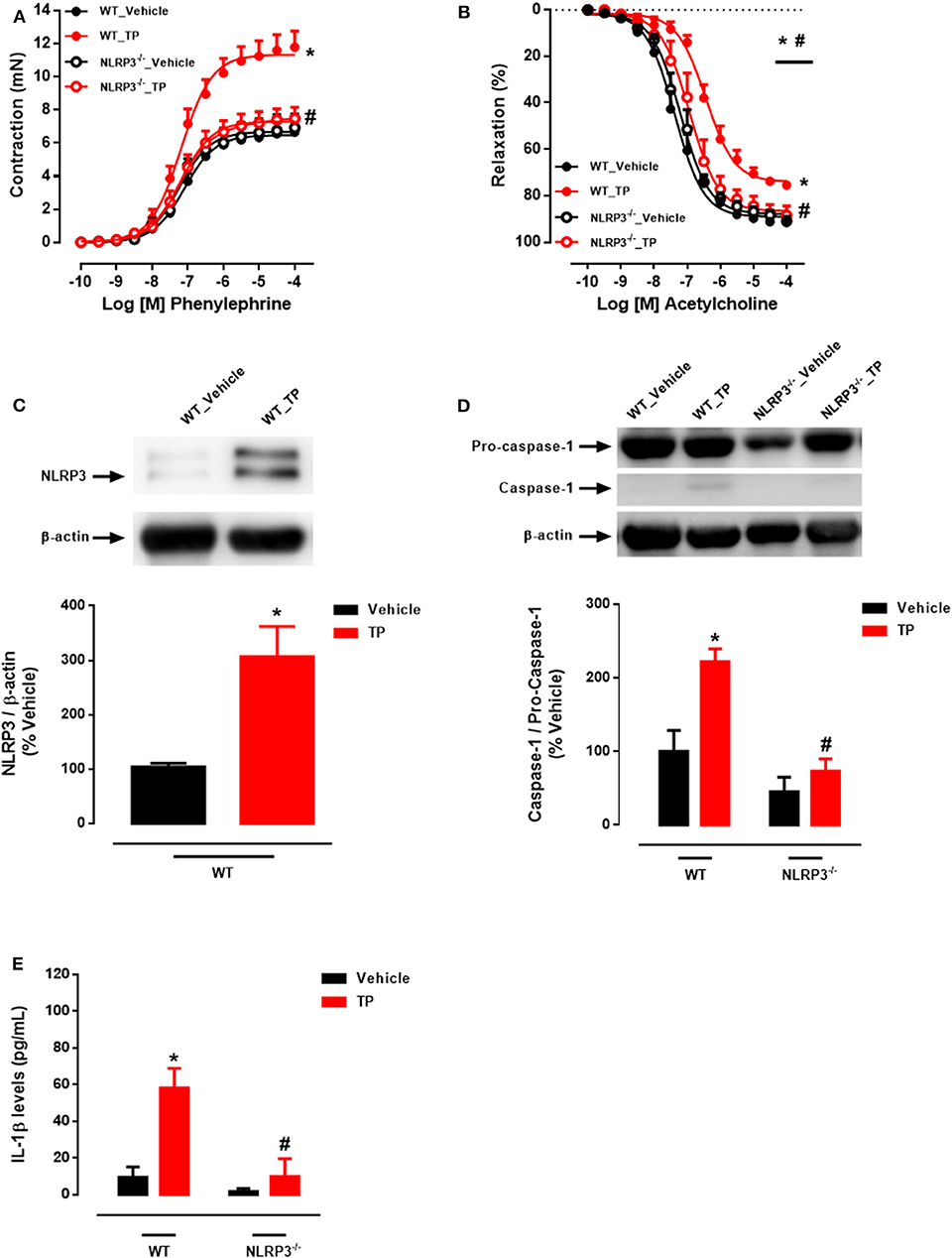
Cardiovascular and Other Risks: Supraphysiological doses are associated with increased risks, particularly cardiovascular. A 2020 study in Frontiers in Immunology found that supraphysiological testosterone levels induced vascular dysfunction via activation of the NLRP3 inflammasome, suggesting potential dose-dependent risks rather than benefits [6 (#citations)]. A 2016 study in Journal of Endocrinologyon rats showed that doses of 5–20 mg/kg induced pathological cardiac hypertrophy, with effects that were not clearly dose-dependent but consistently detrimental [7 (#citations)].To summarize, while muscle-related outcomes show clear dose-dependent benefits, non-muscular outcomes do not consistently demonstrate dose-dependency at supraphysiological levels, and higher doses often increase risks.
More last ditch efforts on your part to try and narrow down the acceptable studies you’ll allow(while countering with rat studies just lmao) so that I don’t have anything to use that you’ll accept as evidence. Like I said in the other thread, the point of a discussion should be to learn, not to win. But since you insist on it being a winner and loser game you should’ve taken the L a long time ago.Cite one that doesn't involve that same comparison to 50 mg TC taken once a week, which is not a physiological protocol.
Now you’re just falling apart. You’ve heard me state repeatedly that lots of people have been harmed by the more is better mentality, including in this very thread. Like I said, you should’ve taken the L a long time ago.Zero. On the contrary, the risk profile goes up while non-muscular benefits are static or retreating. Lipids deteriorate, absolute estradiol can be excessive, HCT goes up, sleep impairment is common.
Ok, ignore the Xyosted data, along with the large quantity of anecdotal evidence showing side effects at higher doses. Continue to deny that the OP and others have been harmed by more-is-better thinking.
") )
)

")








