First off, an advance thank you for the wealth of information I have learned here. I have learned so much browsing as a guest and wish I knew half of what most of you have forgotten.
I am prescribed 200mg/week of Testosterone from my Urologist. I have been on since early 2022.
When tested prior to TRT- I had three tests that all had to be drawn by 8:00AM and my highest was 108ng/dl. Lowest and average was 96ng/dl.
No past drug, anabolics abuse. I drank a lot in my 30’s. Was a little overweight. No injury. The only medical condition is asthma that at times has required a lot of corticosteroid treatments.
Played sports my entire young life and was always strong and naturally more muscular than my peers in my teens and 20’s.
I have had a very stressful personal and professional life.
Started at 150mg/week.. just like everyone else harpooning myself one or twice a week. That got me back to the 700-800ng/dl range.
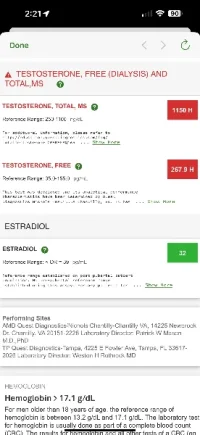
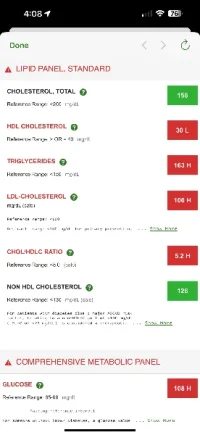
I wanted 900-1100 so he allowed 200mg every 7 days. Then estrogen issues crept up. He prescribed .5mg Armidex to be used when needed but no more often than 4 days. That caused my lipids to get bad. Not horrible but not good either. He prescribed Pravastatin for that.
I changed to daily dosing using an insulin pin. Roughly 180mg/week. Holding around 975ng/dl on average.
Then you can perfectly plot my BP increasing over the last year. Sometimes, shockingly high. He prescribed started hydrochlorthazide and losartin. Now I am only on losartin twice daily.
My questions…
Compared to where I was. 500ng/dl is amazing. But I don’t have the stamina or the strength that I do at 900-100ng/dl. I’m 6’3 and have a lot of mass so I get where I could need (want?) more but is that selfish for a 47 year old? If so, tell me.
I noticed while my strength was going through the roof, I wasn’t adding size other than what I had in my 20’s when still ego lifting. He prescribed Nandrolone which was absolutely amazing. After about a month, I was popping seams in my dress shirts but then came the paranoia and crazy thoughts and I quit it. My brain just couldn’t handle a 19-nor. I was nervous, jealous, paranoid and obsessive.. With this said.. would any of you think it’s normal to want to try Primobolin? (SP) or is that just selfish and stupid?
Testicles.. they are gone. I had good results from HCG but my insurance wouldn’t pay for it and I was tired of shelling out 250 for a vial. But I admit it helped a lot. More than just testicle size. Sensitivity returned, volume of ejaculate was quite impressive, I know.. shallow and petty.
Sensitivity..
5 days out of the week, I can get a great erection and have sex for an hour as hard as I can go. She doesn’t mind but the reason I can go for an hour is that I can’t feel it. The other two days it’s useless which I attribute to the Armidex because I’m just better with my e2 being a little higher. I’m more passionate and friendlier. If it falls below 40 I’m just not really interested in much.
I know I don’t want to be a shell of a man that I was three years ago but for what TRT fixes, it seems to create other issues downstream. For every three months that I’m on top of my game there is a month where I’m just bleh.. is this all worth it? Or does getting old just suck this bad?
Advice? Be honest please. I’m thick skinned and I appreciate your honesty and knowledge!
I am prescribed 200mg/week of Testosterone from my Urologist. I have been on since early 2022.
When tested prior to TRT- I had three tests that all had to be drawn by 8:00AM and my highest was 108ng/dl. Lowest and average was 96ng/dl.
No past drug, anabolics abuse. I drank a lot in my 30’s. Was a little overweight. No injury. The only medical condition is asthma that at times has required a lot of corticosteroid treatments.
Played sports my entire young life and was always strong and naturally more muscular than my peers in my teens and 20’s.
I have had a very stressful personal and professional life.
Started at 150mg/week.. just like everyone else harpooning myself one or twice a week. That got me back to the 700-800ng/dl range.
I wanted 900-1100 so he allowed 200mg every 7 days. Then estrogen issues crept up. He prescribed .5mg Armidex to be used when needed but no more often than 4 days. That caused my lipids to get bad. Not horrible but not good either. He prescribed Pravastatin for that.
I changed to daily dosing using an insulin pin. Roughly 180mg/week. Holding around 975ng/dl on average.
Then you can perfectly plot my BP increasing over the last year. Sometimes, shockingly high. He prescribed started hydrochlorthazide and losartin. Now I am only on losartin twice daily.
My questions…
Compared to where I was. 500ng/dl is amazing. But I don’t have the stamina or the strength that I do at 900-100ng/dl. I’m 6’3 and have a lot of mass so I get where I could need (want?) more but is that selfish for a 47 year old? If so, tell me.
I noticed while my strength was going through the roof, I wasn’t adding size other than what I had in my 20’s when still ego lifting. He prescribed Nandrolone which was absolutely amazing. After about a month, I was popping seams in my dress shirts but then came the paranoia and crazy thoughts and I quit it. My brain just couldn’t handle a 19-nor. I was nervous, jealous, paranoid and obsessive.. With this said.. would any of you think it’s normal to want to try Primobolin? (SP) or is that just selfish and stupid?
Testicles.. they are gone. I had good results from HCG but my insurance wouldn’t pay for it and I was tired of shelling out 250 for a vial. But I admit it helped a lot. More than just testicle size. Sensitivity returned, volume of ejaculate was quite impressive, I know.. shallow and petty.
Sensitivity..
5 days out of the week, I can get a great erection and have sex for an hour as hard as I can go. She doesn’t mind but the reason I can go for an hour is that I can’t feel it. The other two days it’s useless which I attribute to the Armidex because I’m just better with my e2 being a little higher. I’m more passionate and friendlier. If it falls below 40 I’m just not really interested in much.
I know I don’t want to be a shell of a man that I was three years ago but for what TRT fixes, it seems to create other issues downstream. For every three months that I’m on top of my game there is a month where I’m just bleh.. is this all worth it? Or does getting old just suck this bad?
Advice? Be honest please. I’m thick skinned and I appreciate your honesty and knowledge!
")