Keep in mind that although TT is important to know FT is what truly matters as it is the active unbound fraction of T responsible for the positive effects.
Although it is important to know where your trough FT level sits symptom relief is what truly matters.
What level you need to hit would be through trial and error.
Every individual is different as some men will feel good running a mid-range trough whereas others may need a high-end trough to reap the full benefits.
Many tend to aim for a higher-end let alone high trough.
Some will even venture into the absurd territory but that is usually the ones caught up on that more T is better mentality being pushed by those dime a dozen run of the mill T-clinics, so called men's health forums loaded with all those blast n cruizzzers polluting the internet let alone those so called gurus littered on the forums/Gootube!
Unfortunately many men are overmedicated running levels well beyond their genetic set-point.
The goal here is to achieve a healthy trough FT.
Just to put this in perspective most healthy young males would be hitting a FT 10 ng/dL tested using the gold standard Equilibrium Dialysis assay (most accurate) or a cFTV 13-15 ng/dL and this is a short-lived peak to boot!
Trough would be 20-25% lower.
More importantly a FT in the low 20s whether cFTV or standardized ED assay would be very high!
Everyone needs to hammer it in their heads that a trough FT 30 ng/dL is absurdly high.
We are talking f**king TROUGH here too not peak!
Unfortunately many are caught up aiming for that super high FT 30+ ng/dL and this is troughs we are talking about here.
Again big difference between one hitting a very high trough FT 30 ng/dL injecting once weekly vs EOD or daily!
Critical to always pay attention to injection frequency/trough FT level.
Yes many may very well feel better overall running higher-end/high trough FT levels but it is far from a given.
As I have stated numerous times on the forum running too high a FT can be just as bad as running too low a FT in many ways especially when it comes to liibido, erectile function and mood!
Hammering your dopamine from running too high a steady-state/trough FT can easily backfire on you in the long-run.
Everyone has a genetic set-point and unfortunately many end up blowing well beyond it due to being caught upon that more T is better mentality!
Just to be clear here I see no issue if one chooses to run a high-end/high trough FT within reason especially if blood markers are healthy, minus any sides and they feel great overall.
Yes symptom relief is what truly matters but we need to tread lightly when it comes to the cop out for some claiming this is where I feel best!
I could bang 300 mg T/week maybe have minimal sides, blood markers fairly good overall other then very
high hematocrit yet state this is where I feel best.
When you seen how absurd my TT and more importantly trough FT levels were on such protocol they would be well past therapeutic!
Such dose would never be needed to achieve a healthy let alone high trough FT level let alone experience relief/improvement of low-T symptoms.
Also remember when first starting TTh or tweaking a protocol (increasing/decreasing T dose) hormones will be in FLUX during the weeks leading up until blood levels have stabilized (4-6 weeks TE/TC) and it is common to experience ups/downs during the transition as the body is trying to adjust.
Even then once blood levels have stabilized it will still take the body time (a few more months) to adapt to its new set-point and this is the CRITICAL time period when one needs to gauge how they truly feel overall regarding relief/improvement of low-T symptoms and overall well-being!
The first 6 weeks means nothing when looking at the bigger picture here.
Every protocol needs to be given a fighting chance (12 weeks) before claiming whether it was truly a success or failure!
If you jump the gun too soon which many of the misinformed do then you will be left chasing your tail endlessly caught up on that never-ending merry go round!
Again patience is key.
Have realistic expectations especially when it comes to libido and erectile function!
Just to be clear up any confusion this is Fiers camps data for mFT reference ranges not the harmonized reference range being worked on by the CDC. *Serum samples were analyzed from healthy men participating in the SIBLOS/SIBEX and EMAS studies, both population-based cohort studies * mFT...

www.excelmale.com
*We established mFT reference ranges for healthy men aged 18 to 69 years
We present 95% mFT age-stratified reference ranges
Age category (years)
|
Median mFT (ng/dl)
|
95% mFT reference range (ng/dl)
|
25-29 (n=148)
|
10.3
|
5.6 - 17.1
|
30-39 (n=252)
|
9.7
|
4.9 - 18.1
|
40-49 (n=207)
|
8.0
|
4.3 - 13.5
|
50-59 (n=146)
|
7.0
|
3.8 - 12.6
|
60-69 (n=114)
|
5.9
|
3.3 - 11.9
|
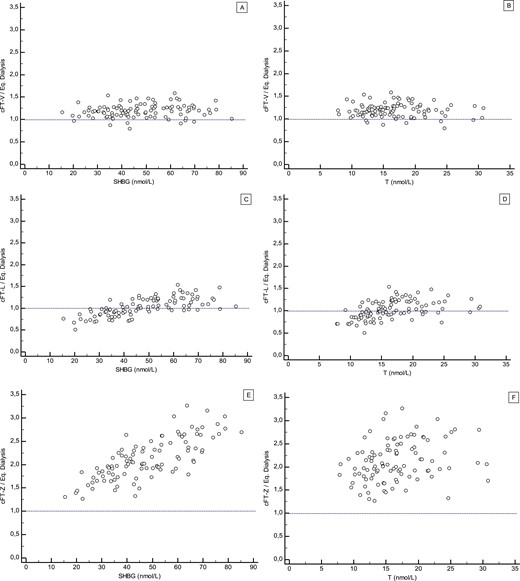
*The gold-standard for the determination of FT levels is considered to be directly measured free testosterone (mFT) using equilibrium dialysis followed by mass spectrometry (ED LC-MS/MS). However, no widely accepted reference ranges are available for this clinical parameter. We established mFT reference ranges for healthy men aged 18 to 69 years
*Serum samples were analyzed from healthy men participating in the SIBLOS/SIBEX and EMAS studies, both population-based cohort studies
* mFT levels were measured in 867 men using ED LC-MS/MS as previously reported (1).
Reference: 1. Fiers T, Wu F, Moghetti P, Vanderschueren D, Lapauw B, Kaufman JM.
Reassessing Free-Testosterone Calculation by Liquid Chromatography–Tandem Mass Spectrometry Direct Equilibrium Dialysis. J Clin Endocrinol Metab. 2018;103(6). doi:10.1210/jc.2017-02360
Reassessment of FT in women and men with state-of-the-art methodology confirms previously established FT percentages but highlights limitations of differen

academic.oup.com
In the current study, we used a state-of-the-art direct ED method to reassess FT in sets of representative serum samples. This method takes advantage of the ability of a highly sensitive and accurate measurement of T by liquid chromatography–tandem mass spectrometry (LC-MS/MS) to reliably measure the low FT concentration directly in the dialysate after ED. This more straightforward method avoids potential sources of inaccuracy in indirect ED, such as those resulting from tracer impurities or from measures to limit their impact (e.g., sample dilution). We then used the measured FT results to re-evaluate some characteristics of two more established and a more recently proposed calculations for estimation of FT.
Again would tread lightly on how high you run your trough/steady-state FT level! This can easily backfire in the long-run for many especially when it comes to mood, libido and erectile function! Too high a FT level can be just as bad in many ways as having too low a FT level. Libido starts in...
www.excelmale.com
https://www.yahoo.com/lifestyle/truth-testosterone-libido-185000725.html?soc_src=social-sh&soc_trk=tw&tsrc=twtr As an expert on andrology and sexual dysfunctions, urologist Andrew Y. Sun, M.D., sees plenty of patients who’re struggling with low libido. And most are pretty sure they...
www.excelmale.com