madman
Super Moderator
PDF (pp.176-199)

INTRODUCTION
Sex steroids are main drivers of sexual development and play a fundamental role in many physiological processes in both men and women [1,2]. As such, alterations in sex steroid exposure can have significant consequences as seen in men with hypogonadism or in women with hyperandrogenism [3,4]. Therefore, it is important to accurately quantify sex steroid hormone concentrations to correctly diagnose related pathologies. Commonly, total serum sex steroid concentrations are used as a measure of exposure. However, the free hormone hypothesis suggests that free steroid concentrations better reflect cellular action and thus sex steroid exposure as only these fractions can freely cross the cell membrane [5,6]. This has for example been suggested for free testosterone (T) in men [7–9] and usage of free T estimates alongside total T measurements has already been included in clinical guidelines[10,11]. Nevertheless, measuring free T concentrations is challenging as only 1-2% of the total T fraction is free. Only specialized techniques such as equilibrium dialysis followed by liquid chromatography tandem mass-spectrometry (ED LC-MS/MS) can measure these low concentrations[12]. As most laboratories do not have access to sufficiently sensitive techniques, they need to rely on calculations to estimate free sex steroid concentrations from sex hormone binding globulin (SHBG), albumin and total sex steroid concentrations [13–15].
One drawback of these calculators is that the binding affinity is often assumed to be constant, whereas it may be partly dependent on SHBG and sex hormone concentrations [16]. Other factors can also influence the affinity such as variations in protein structure or non-specific competitive binding. Earlier studies have identified several single-nucleotide polymorphisms (SNPs) that potentially affect the binding of sex hormones to SHBG and/or concentrations of SHBG or total T. Most of these SNPs are present in or near the SHBG gene, though one that affects only total T is on the X-chromosome [17–20]. Two, rs6258 and rs6259, are located in the coding region of the SHBG gene and induce a structural mutation within the protein thereby perhaps altering its binding affinity [17]. If this is so, these SNPs could affect the performance of free sex steroid calculators. A first element potentially decreasing their performance in SNP-carriers is the introduction of bias due to a difference between the actual binding affinity and the one used in calculators. A second issue is that routine SHBG measurements are currently performed using immunoassays. Coding SHBG SNPs may alter the epitope to which the antibodies bind, resulting in an altered binding in the immunoassay and ultimately to under- or overestimation of the SHBG concentrations and subsequent over- or underestimation of free sex steroid concentrations.
To overcome the potential bias of immunoassays resulting from SHBG mutants, we used an LC-MS/MS method that allows for SHBG quantification while discriminating structural rs6258 SHBG mutants from wild-type (WT) SHBG [21]. In this study, we will evaluate the effects of SNPs that are suggested to affect SHBG concentration or structure of SHBG on total and free T concentrations. Moreover, we investigate how these SNPs affect calculator performance as compared to direct measurements of free T concentrations. Additionally, we will compare performance and discriminatory potential of the LC-MS/MS method against SHBG immunoassays in samples of rs6258 and rs6259 carriers.
MATERIALS AND METHODS
Study population
Serum samples were obtained from healthy men participating in the SIBLOS study. This study is a population-based sibling-pair study investigating sex hormone status, body composition and bone metabolism as well as possible determinants thereof in 999 healthy men aged 25-45 years old. The studies involving different SHBG assays were performed in samples obtained in a SIBLOS follow-up, the SIBEX study. For detailed description of the SIBLOS/SIBEX studies we refer to earlier work [22].All analyses were approved by the ethics committee of Ghent University Hospital (2001/60, 2013/1090).
Genotyping
Subjects were genotyped using an Illumina® (Illumina, San Diego, CA)microarray (Infinium® Global Screening Array-24 V1.0) for SNPs which are suggested to affect binding affinity and/or the concentration of SHBG or total T (rs6258, rs6259, rs1799941, rs12150660, rs727428, rs5934505).
Hormonal measurements
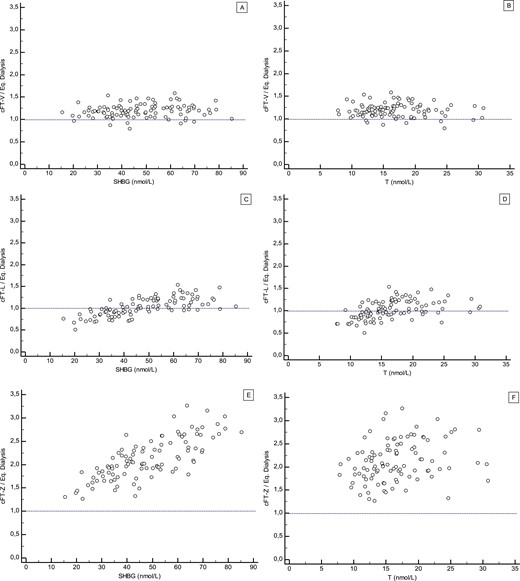
Venous blood samples were taken between 8:00 and 10:00 in the morning after overnight fasting. Concentrations of serum total T were measured by LC-MS/MS as described previously (inter-assay CV at 104 pmol/L:6.5%; LOQ: 35 pmol/L) [22]. Free T concentrations were calculated from serum total T, SHBG and albumin using an equation based on the law of mass action according to Vermeulen et al. [13]. Additionally, in a randomly selected subset (n = 314) free T concentrations were directly measured using equilibrium dialysis followed by LC-MS/MS (inter-assay CV at 150 pmol/L: 10.6%; LOQ: 2.4 pmol/L) following earlier described methodology [12]. SHBG serum concentrations were determined by electrochemiluminescence immunoassay using the Cobas e801 (Roche Diagnostics, Indianapolis, IN) (CV: 7.22% at 18.15 nmol/L). Additionally, to evaluate the effects of structural mutants on SHBG measurements, a subset was randomly selected of samples from 8 men for every structural mutant genotype in our population (rs6258 heterozygous,rs6259 heterozygous and rs6259 homozygous) and WT controls. In this subset, SHBG concentrations were also measured using the Abbott Alinity immunoassay (Abbott Laboratories, North Chicago, IL) (CV: 1.99% at 8.31nmol/L; 5.27% at 28.34 nmol/L) and the LC-MS/MS method described below.
SHBG measurement by LC-MS/MS.
The stable-isotope labeled (SIL) internal standard peptide LLLVPALDGC (CAM) LR, purity: 98.6%, with a carbamidomethylated (CAM) cysteine and a 13C6 15N4-labeled C-terminal arginine, further referred to as LLLVPALDGCLR-SIL, was custom synthesized by Pepscan (Lelystad, The Netherlands). Other chemicals, materials and sample pretreatment were as previously described [21].
Wild-type SHBG concentrations were determined by measuring the concentration of three different, SHBG-specific peptides using LC-MS/ MS: TSSSFEVR, IALGGLLFPASNLR and LPLVPALDGCLR (highest CVs: 3.9% at 14.4 nmol/L, 1.9% at 14.9 nmol/L and 1.8% at 15.2 nmol/L for the TSSSFEVR, IALGGLLFPASNLR and LPLVPALDGCLR peptides, respectively). Rs6258 (P156L) mutated SHBG concentrations were determined by measuring the concentration of the mutated peptide LLLVPALDGCLR. Any difference in concentration between total and wild-type specific SHBG in a sample must be attributed to the presence of one or more isoforms of this protein which do not have the exact LPLVPALDGCLR sequence in their structure, such as the isoform with the rs6258 mutation. Peptide specific detection parameters for peptide LLLVPALDGCLR and its internal standard are presented in Supplementary table 1. Other chromatography and detection settings were used as previously described [21]. Briefly, SHBG and other endogenous proteins were isolated from 50 µL of sample by precipitation with 200 µL of 1% trichloroacetic acid in 2-propanol and centrifugation. The supernatant was discarded. The obtained protein pellet was resuspended and digested for 3 hours at 37 ºC by a trypsin solution (150 µg/mL trypsin in 50 mM ammonium bicarbonate buffer with 5% acetonitrile), after addition of 20 µL of a solution containing the four SIL internal standard peptides. Next, the samples were reduced (with dithiothreitol), alkylated (with iodoacetamide) and acidified (with formic acid). Aliquots of 2 µL of the digests were analyzed by liquid chromatography on a 100x1.0 mm C18 column (1.6 µm particles) at 60 ºC and a 17-min gradient of 0.1% formic acid in water and 0.1% formic acid in acetonitrile at 80 µL/min. Detection of four of the generated SHBG-specific peptides and their SIL internal standards was performed by positive electrospray ionization tandem mass spectrometry. SHBG concentrations in patient samples were determined by reference to a similarly treated calibration curve of purified human SHBG spiked into a 1:1 (v/v) mixture of rat serum and phosphate buffered saline across the concentration range of 200 to 20,000 ng/mL.
Statistical analysis
All statistics were performed using the RStudio program version 4.3.0 (Rstudio, Boston, MA, USA) and Graphpad Prism version 9.1.0 (Graphpad Software, Boston, MA, USA). The SNPs of interest were analyzed for Hardy-Weinberg equilibrium by comparing the expected and observed prevalence of SNPs using chi-square tests. Linkage between the SNPs was determined using the LDlinkR package. This package accesses the 1000 genomes database of which the EUR (European) population was used as a representative population to determine linkage disequilibrium. Afterwards, effects of the SNPs on hormonal parameters were modelled using random intercept linear mixed modelling with all SNPs except rs12150660 as fixed effects, family number as a random effect, and corrected for age and BMI. Additionally, linear mixed modelling analysis was performed to identify potential measurement differences between assays for structural SHBG mutants. The effects of the different SNPs on SHBG assay agreement were determined using a model containing the group (WT, rs6258 heterozygous, rs6259 heterozygous and rs6259 homozygous) and assay as well as their interaction as fixed effects and sample ID as random effect. These interaction terms allow detection of a difference in mean SHBG concentration for a given method in different groups. The WT group and Roche immunoassay were set as the references for the group and assay parameter respectively. Additionally, a linear mixed model was fit modelling SHBG concentrations in function of rs6258 and rs6259 with an interaction term to determine whether rs6258 carriers with the rs6259 SNP could be included in the rs6258 group. All models were generated using the lme4 package using restricted maximum likelihood parameter estimation and an unstructured covariance matrix. P-values ≤ 0.05 were considered significant.
RESULTS
General characteristics of the study population
General characteristics and sex steroid concentrations of the SIBLOS/ SIBEX participants were published previously [22]. In brief, the mean age of the SIBLOS population was 34 ± 6 years with a follow-up visit (SIBEX) after an average of 12 ± 2 years. Mean BMI was 25.1 (95% CI: 24.8-25.4). General characteristics of the subset of participants whose samples were subjected to LC-MS/MS SHBG measurements can be found in Supplementary table 2. WT subgroup did not differ significantly from the general SIBEX population in age and BMI.
SNP prevalence, Hardy-Weinberg equilibrium and linkage
Of the analyzed samples, 10 had a sample call rate below 97.5% and were not included in the analysis. The allelic prevalence of the SNPs of interest in the SIBLOS (n = 989) population can be found in Table 1. Supplementary figure 1 shows the overlap between SNPs in this population: only 82 (8%) individuals had no SNP of interest and 434 (43%) individuals only had 1 SNP. No SNPs deviated significantly from Hardy-Weinberg equilibrium. Significant linkage affecting statistical analysis was observed between rs12150660 and rs1799941 (R² = 0.90, p: <0.001), so that rs12150660 was not used in further analyses and all results for rs1799941 should be interpreted as a combined effect of both SNPs. Significant, but not disturbing, linkage was also observed between rs727428 and three other SNPs: rs6259 (R² = 0.15, p: <0.001), rs1799941 (R² = 0.25, p: <0.001) and rs12150660 (R² = 0.22, p: <0.001).
Hormonal parameters
Results of linear mixed modelling analyses for SHBG, total and calculated free T can be found in Table 2 and an analysis comparing directly measured and calculated free T in a subset of 314 individuals in Table 3. In the larger study population, multiple significant associations were found between SNPs and serum SHBG and testosterone concentrations. Rs6258 heterozygosity was associated with lower SHBG concentrations (-9.6 nmol/L; -24.7%), while rs6259 heterozygosity, rs727428 homozygosity and rs1799941 hetero- or homozygosity were associated with higher SHBG concentrations (+4.2 to 9.0 nmol/L; +10.8 to 23.1%). The presence of rs727428 homozygosity, rs6259, rs179994 or rs5934505 was associated with higher concentrations of total T (+0.79 to 4.36 nmol/L; 3.9 to 21.4%). Calculated free T levels were higher in rs6259 homozygotes (+72.7 pmol/L; +18.7%) and rs5934505 carriers (+17.0 pmol/L; +4.4%). Rs6258 heterozygosity was associated with a higher percentage calculated free T (2.23%) while rs6259 heterozygosity, and rs1799941 and rs727428 heteroor homozygosity were associated with a lower percentage calculated free T (1.77 and 1.90%, respectively) compared to the population mean (1.97%)
In the subset of 314 subjects, findings for SHBG and total T concentrations as well as for percentage free T were similar to those observed in the larger study population. For both measured and calculated free T, SNP carriers were not different from the population mean although a similar but non-significant trend towards higher free T levels was observed for rs6259 homozygotes. In this subset, no significant associations were found between the SNPs and the expected difference between measured and calculated free T.
SHBG assay comparison
In general, the LC-MS/MS-derived SHBG concentrations (for all three signature peptides) in the analyzed subgroup are 15-20% lower than those found with the immunoassays (Fig. 1). Interaction terms between the SNP groups and the assays of the SHBG measurements are shown in Supplementary table 4 for the subset of 32 samples subject to LC-MS/ MS SHBG measurement. The LLLVPALDGCLR peptide was not included in this analysis due to multicollinearity issues with the other peptides, specifically LPLVPALDGCLR. Significant interaction terms, indicating a significant change in the expected difference between the Roche immunoassay and another assay due to a SNP, were observed for all LC-MS/MS peptide measurements in the rs6259 homozygous group (all p<0.001) as well as for the LPLVPALDGCLR-peptide measurement in the rs6258 heterozygous group (p<0.001).
Occurrence of P156L SHBG in serum
Next to the three peptides that are present in wild-type SHBG, one additional peptide was included in the LC-MS/MS method: LLLVPALDGCLR which is the predicted sequence within SHBG in case of the rs6258 SNP (substitution of proline at position 156 by leucine, P156L). While an extensive method validation for the other three peptides has previously shown the quantitative reliability of the LC-MS/MS method [21], no reference material is available for intact SHBG with the P156L mutation. As such, the concentration of this protein isoform cannot be quantitatively determined. Alternatively, the reproducibility of the determination of this peptide was investigated by analyzing three serum samples from individuals with the rs6258 SNP each in triplicate on three different days. The precision of the entire methodology, including extraction, digestion and LC-MS/MS analysis, expressed as the coefficient of variation over 9 determinations of the peak area ratio of the peptide relative to its internal standard, was <5% for all samples (Supplementary table 3). Figure 2 shows the response (peak area ratio of peptide over internal standard) for total SHBG set at 100% based on the mean values of the signature peptides TSSSFEVR and IALGGLLFPASNLR, together with the relative amounts of wild-type SHBG (based on the response of peptide LPLVPALDGCLR) and of SHBG with the P156L mutation (based on the response of peptide LLLVPALDGCLR) for serum samples from eight individuals heterozygous for the rs6528 SNP. The percentages of P156L SHBG expressed in these individuals ranged from 14.1 to 19.2%, which is of similar magnitude as the calculated differences between total and wild-type SHBG serum concentrations in these individuals. This P156L expression is remarkably lower than expected, as theoretically the percentage of P156L expression would be 50% of all SHBG.
DISCUSSION
This study investigated SNPs that are suggested to affect SHBG or T concentrations or the affinity of SHBG for T. We evaluated the prevalence of these SNPs in a healthy male population and their effects on SHBG, total T and both directly measured as well as calculated free T serum concentrations. To further deepen our insight into how structural mutants affect free T we also performed SHBG measurement using an LC-MS/MS method capable of detecting P156L SHBG in serum.
Firstly, our results show that SNPs that potentially affect sex steroid or SHBG concentrations or SHBG’s affinity for sex steroids are relatively common in a healthy male population and are in line with prevalences described in earlier studies [18,23–25]. Additionally, no SNPs deviate from Hardy-Weinberg equilibrium suggesting that no major genetic effects, such as inbreeding or selection, are affecting our study population.
Structural mutations (rs6258 and rs6259) were relatively less common than non-coding mutations. Especially rs6258 was rare, with an allelic prevalence of only 0.5%. The exact reason for this low prevalence is unclear. It must be considered that our study only included healthy, young men so that individuals in whom a SNP has caused disease might have been excluded from this study
Secondly, our results are also largely in line with earlier literature showing, for example, lower (total) SHBG serum concentrations in individuals with rs6258 [18] and higher SHBG concentrations in rs6259 heterozygous individuals [26]. However, our results show no substantial effects of most of these SNPs on free T concentrations. This indicates an only limited effect, if any, of the SHBG SNPs on free T concentrations and is compatible with the view that it is the free T concentration that is primarily determined through hypothalamic-pituitary feedback regulation, which annuls the effects of altered SHBG binding on free T concentrations in healthy men. The higher total T concentrations without concomitant higher free T which we observed for several SNPs also suggest that clinical decisions based on total T concentrations alone may lead to a potentially incorrect diagnosis of hypogonadism in carriers of these SNPs.
There was a trend towards higher free T concentrations observed in rs6259 homozygous carriers, which was significant only in the larger dataset (n = 989) for calculated free T. However, this is unlikely to greatly affect the use of calculated free T in clinical practice as this genotype only occurs in 1.4% of the population (Table 1). Our results also confirm that the binding affinity is altered in heterozygous rs6258 carriers, manifesting in a higher percentage measured free T in these individuals, albeit maybe to a lesser extent that what would be expected from experimental studies [17,18]. Further, no effects of SNPs were observed on the difference between calculated and measured free T, indicating a minimal effect of SNPs on calculator performance. Rs5934505 served as a control for calculator performance, confirming the expected higher free T but non-affected percentage free T in carriers of this SNP which causes higher total T but non-affected SHBG concentrations.
Finally, we assessed the ability of different SHBG assays, immunoassays and LC-MS/MS, to detect and differentiate between structural mutants of the SHBG protein. We observed average differences between immunoassays and LC-MS/MS (15-20% lower for LC-MS/MS) similar to those reported earlier [21]. The exact reason for this difference is unclear, but is possibly related to differences in binding between endogenous SHBG and the spiked SHBG standard by the antibodies used in the immunoassays, an issue that the antibody-free LC-MS/MS method does not have. It is remarkable that such a difference was not found between SHBG concentrations measured by LC-MS/MS and the immunoassays for the rs6259 homozygous individuals. This may be related to the substitution of aspartic acid at position 327 by asparagine in the SHBG molecule because of the extra N-linked glycosylation site introduced by this SNP [17,26]. This site may influence the binding between SHBG and antibody in the immunoassay [27,28]. The fact that there still was a difference between LC-MS/MS and immunoassays for the individuals with a rs6259 heterozygous SNP, just like for the wildtype group, is probably because of the presence of higher concentrations of non-mutated SHBG in these heterozygotes. Within the group with the rs6258 SNP, the wild-type specific LPLVPALDGCLR signature peptide showed a lower concentration than the other two generic peptides, which is expected as this SNP leads to the proline within the LPLVPALDGCLR peptide being substituted by a leucine at the 156 position [26,29]. As there is no reference material for intact SHBG with the P156L mutation, only the reproducibility of the determination of SHBG via signature peptide LLLVPALDGCLR could be assessed. Since the overall coefficient of variation was <5%, the method showed good reproducibility for the analysis of mutated SHBG using the LLLVPALDGCLR peptide (Supplementary table 3). Also, the percentage of mutated SHBG measured in serum samples from eight rs6258 carriers was similar to the calculated differences between total and wild-type SHBG (Fig. 2). First of all, this confirms that SHBG with the P156L mutation actually occurs in the circulation of individuals with this particular SNP. However, since its proportion is below 20% of total SHBG (and not the expected 50% mutation rate of all SHBG molecules) this explains why we found it not to greatly affect calculated estimates of free T, despite the reported markedly reduced affinity for T [17,18]. This concentration gap could potentially be attributed to a poorer production or excretion of the mutant protein, a faster degradation, or a combination of both. A plausible mechanistic explanation for this observation is that P156 is located subsequent to a beta-sheet in the wild-type (WT) SHBG structure. It is probable that P156 serves as a pivotal structural disruptor, playing a critical role in achieving and preserving the correct tertiary structure. Substituting this position with a leucine residue, which possesses distinct biochemical properties, is likely to impact the folding process and the stability of the P156L SHBG variant. As this lower mutant peptide is comparably lower among all 8 carriers (data not shown) and the SHBG gene is not known to be imprinted, genetic imprinting is a less likely explanation. However, more research is required to elucidate the exact molecular mechanisms responsible for these low concentrations of mutant SHBG. Secondly, the fact that measured P156L SHBG corresponds well to the difference between total and wild-type SHBG is an indication of equivalent analytical behavior of the wild-type and mutated forms of this protein, in terms of extraction, digestion and further analysis using LC-MS/MS, and is an additional sign of method reliability
Some strengths and limitations of this study have to be kept in mind. One strength of this study is its well-characterized population and population size. 999 healthy men were included in the study, of which 989 were successfully genotyped, allowing for thorough examination of the in vivo effects of SNPs. However, rarer genotypes (rs6258 heterozygosity and rs6259 homozygosity) were only present in low numbers (14 and 12 individuals respectively), limiting the power of statistical analyses. The statistical analyses also simplified the effects of genetic variation to average effects for every SNP. In reality, individuals often carry multiple SNPs and the effects on SHBG and/ or T levels will depend on the number and combination of SNPs and potential synergistic or antagonistic effects of SNPs on each other. Importantly, the presented findings in men cannot be extrapolated to women in whom the regulation of total and free T concentrations, and thus the expected effects of the SNPs on hormonal levels, differs profoundly from those in men. Further, some findings may not apply to diseased men with altered free T regulation. A strength of the study is the inclusion of a reference method for the measurement of free T allowing to establish the actual effects of SNPs on free T and a reliable comparison with calculated free T. Finally, the inclusion of a novel, LC-MS/MS-based method for the measurement of SHBG allowed the specific detection of P156L SHBG in serum samples of rs6258 carriers, enabling evaluation of in vivo expression of P156L SHBG. Additionally, the antibody-independent design of this method allowed us to identify a potential effect of rs2659 homozygosity on antibody binding to SHBG.
CONCLUSION
In this study, we have shown that SNPs that potentially affect SHBG concentration or binding affinity for sex steroids are common in a population of healthy men but that effects of these SNPs on SHBG and testosterone concentrations were mostly mild. In contrast, directly measured free T concentrations were unaffected as were also the differences between measured and calculated free T. Further, we have also demonstrated the potential of LC-MS/MS to detect mutant P156L SHBG. We found that P156L SHBG is indeed present in the serum of mutation carriers, albeit in lower concentration than expected. In conclusion, free T measurements and calculations appear less affected by variations induced by SNPs compared to total T measurements. As such, clinical decision making based on total T may be more vulnerable to the effects of SNPs while no extra measures should be taken when using the calculations in SNP carriers.