BadassBlues
Well-Known Member

Study Finds Way to Reverse Alzheimer’s - Neuroscience News
Researchers showed that a severe drop in NAD+—a core energy molecule—drives Alzheimer’s pathology in both human brains and mouse models.
Summary: A new study challenges the long-held belief that Alzheimer’s disease cannot be reversed. Researchers showed that a severe drop in NAD+—a core energy molecule—drives Alzheimer’s pathology in both human brains and mouse models.
Restoring proper NAD+ balance with the drug P7C3-A20 not only prevented disease in at-risk mice but also reversed advanced pathology, repairing brain damage and fully restoring cognitive function. The findings point to a major shift in how Alzheimer’s may be treated, suggesting that recovery—not just slowing decline—could one day be achievable.
Key Facts
- Central NAD+ Failure: Human and mouse Alzheimer’s brains showed a dramatic loss of NAD+, impairing essential cellular functions.
- Reversal Achieved: Restoring NAD+ balance repaired pathology and fully recovered cognition even in mice with advanced disease.
- New Treatment Pathway: The targeted drug P7C3-A20 restored healthy NAD+ levels without the dangers linked to over-the-counter NAD+ boosters.
Source: University Hospital Cleveland Medical Center
For over a century, Alzheimer’s disease (AD) has been considered irreversible. Consequently, research has focused on disease prevention or slowing, rather than recovery.
Despite billions of dollars spent on decades of research, there has never been a clinical trial of a drug for AD with an outcome goal of reversing disease and recovering function.
Now, a research team from University Hospitals, Case Western Reserve University, and the Louis Stokes Cleveland VA Medical Center has challenged this long-held dogma in the field. They tested whether brains already badly afflicted with advanced AD could recover.
The study, led by Kalyani Chaubey, PhD, from the Pieper Laboratory, published today in Cell Reports Medicine.
Through studying diverse preclinical mouse models and human AD brains, the team showed that the brain’s failure to maintain normal levels of a central cellular energy molecule, NAD+, is a major driver of AD, and that maintaining proper NAD+ balance can prevent and even reverse the disease.
NAD+ levels decline naturally across the body, including the brain, as people age. Without proper NAD+ balance, cells eventually become unable to execute critical processes required for proper functioning and survival.
In this study, the team showed that the decline in NAD+ is even more severe in the brains of people with AD, and that this also occurs in mouse models of the disease.
While AD is a uniquely human condition, it can be studied in the laboratory with mice that have been engineered to express genetic mutations that cause AD in people. The researchers used two of these models.
One line of mice carried multiple human mutations in amyloid processing, and the other mouse line carried a human mutation in the tau protein.
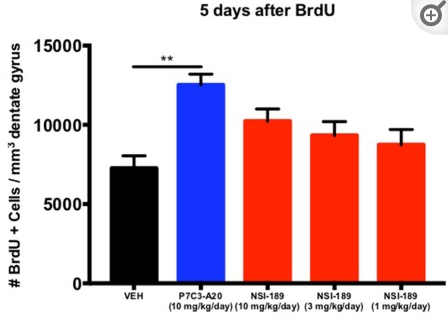
Amyloid and tau pathology are two of the major early events in AD, and both lines of mice develop brain pathology resembling AD, including blood-brain barrier deterioration, axonal degeneration, neuroinflammation, impaired hippocampal neurogenesis, reduced synaptic transmission, and widespread accumulation of oxidative damage.
These mice also develop severe cognitive impairments that resemble what is seen in people with AD.
After finding that NAD+ levels in the brain declined precipitously in both human and mouse AD, the research team tested whether preventing the loss of brain NAD+ balance before disease onset or restoring brain NAD+ balance after significant disease progression, could prevent or reverse AD, respectively.
The study was based on their previous work, published in Proceeding of the National Academy of Sciences USA, showing that restoring the brain’s NAD+ balance achieved pathological and functional recovery after severe, long-lasting traumatic brain injury.
They restored NAD+ balance by administering a now well-characterized pharmacologic agent known as P7C3-A20, developed in the Pieper lab.
Remarkably, not only did preserving NAD+ balance protect mice from developing AD, but delayed treatment in mice with advanced disease also enabled the brain to fix the major pathological events caused by the genetic mutations. Moreover, both lines of mice fully recovered cognitive function.
This was accompanied by normalized blood levels of phosphorylated tau 217, a recently approved clinical biomarker of AD in people, providing confirmation of disease reversal and highlighting a potential biomarker for future clinical trials.
“We were very excited and encouraged by our results,” said Andrew A. Pieper, MD, PhD, senior author of the study and Director of the Brain Health Medicines Center, Harrington Discovery Institute at UH.
“Restoring the brain’s energy balance achieved pathological and functional recovery in both lines of mice with advanced Alzheimer’s. Seeing this effect in two very different animal models, each driven by different genetic causes, strengthens the idea that restoring the brain’s NAD+ balance might help patients recover from Alzheimer’s.”
Dr. Pieper also holds the Morley-Mather Chair in Neuropsychiatry at UH and the CWRU Rebecca E. Barchas, MD, DLFAPA, University Professorship in Translational Psychiatry. He serves as Psychiatrist and Investigator in the Louis Stokes VA Geriatric Research Education and Clinical Center (GRECC).
The results prompt a paradigm shift in how researchers, clinicians, and patients can think about treating AD in the future.
“The key takeaway is a message of hope – the effects of Alzheimer’s disease may not be inevitably permanent,” said Dr. Pieper. “The damaged brain can, under some conditions, repair itself and regain function.”
Dr. Chaubey further explained, “Through our study, we demonstrated one drug-based way to accomplish this in animal models, and also identified candidate proteins in the human AD brain that may relate to the ability to reverse AD.”
Dr. Pieper emphasized that currently available over the counter NAD+-precursors have been shown in animal models to raise cellular NAD+ to dangerously high levels that promote cancer.
The approach in this study, however, uses a pharmacologic agent (P7C3-A20) that enables cells to maintain their proper balance of NAD+ under conditions of otherwise overwhelming stress, without elevating NAD+ to supraphysiologic levels.
“This is important when considering patient care, and clinicians should consider the possibility that therapeutic strategies aimed at restoring brain energy balance might offer a path to disease recovery,” said Dr. Pieper.
This work also encourages new research into complementary approaches and eventual testing in patients, and the technology is being commercialized by Cleveland-based company Glengary Brain Health, co-founded by Dr. Pieper.
“This new therapeutic approach to recovery needs to be moved into carefully designed human clinical trials to determine whether the efficacy seen in animal models translates to human patients,” Dr. Pieper explained.
Additional next steps for the laboratory research include pinpointing which aspects of brain energy balance are most important for recovery, identifying and evaluating complementary approaches to Alzheimer’s reversal, and investigating whether this recovery approach is also effective in other forms of chronic, age-related neurodegenerative disease.”
Key Questions Answered:
Q: What did researchers discover about NAD+ in Alzheimer’s disease?A: They found that a severe decline in NAD+ is a major driver of Alzheimer’s pathology, disrupting energy balance and damaging key brain systems.
Q: Can restoring NAD+ actually reverse advanced Alzheimer’s effects?
A: Yes. In two distinct Alzheimer’s mouse models, restoring NAD+ balance repaired structural and functional brain damage and fully restored cognitive performance.
Q: Why is P7C3-A20 different from common NAD+ supplements?
A: Over-the-counter NAD+ precursors can push NAD+ to unsafe levels, but P7C3-A20 helps the brain maintain proper NAD+ balance under stress without causing harmful elevations.



 medchemexpress.com
medchemexpress.com