Hi, I'm new to the forum and new to try. In 2023 I was diagnosed with low testosterone and was prescribed a topical testosterone gell which didn't work. In fact my counts got lower after using it. So I went to a urologist and he ran some tests and decided I was a candidate for trt via cypionate. I was prescribed 100mg 1x per week intramuscular injections. My starting t was 121 and estradiol was 17.7. My 6 week blood work was 873T and 49.7 estradiol 5 days after my last shot. So I would assume that at some point I may have gotten to around 1000T before it started to fall off. I have a couple questions.
1. Should my Dr test my sbgh, because he hasn't.
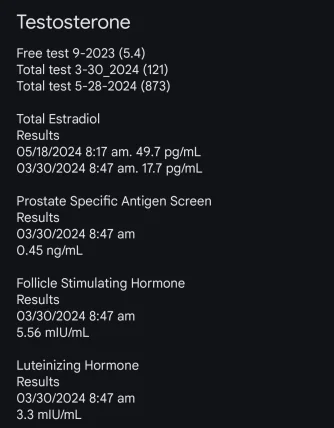
2. Should he check my free testosterone, because he hasn't. My previous NP did prior to the gell and it was 5.4.
3. I'm at week 8 and haven't had much change in mood, libido or energy. Would 2x per week help me there? Could I be getting too much at once? He said that the estradiol was not concerning.
4. I've decided to do 50mg every 3.5 days to see if it helps. What will that do to my testosterone numbers? Will I still get up to around 1000 doing it that way or will it keep me lower but without the peaks and valleys?
5. I am not on any kind of blockers because he didn't see any harmful side effects yet. Is the estradiol a concern at those numbers?
Thanks in advance for any info that you can give.
My starting t was 121 and estradiol was 17.7. My 6 week blood work was 873T and 49.7 estradiol 5 days after my last shot. So I would assume that at some point I may have gotten to around 1000T before it started to fall off.
100 mg TC/TE is a common starting dose.
Downfall when injecting once weekly is there will be a big difference in the peak--->trough and blood levels will not be as stable throughout the week.
Your T level will be at its highest point during your peak (8-12 hrs) post-injection/during the first 2-3 days every week only to be followed by lower levels come weeks end.
For many this can have a negative impact on mood, energy, libido and erectile function due to the rollercoaster type effect.
Easy way to remedy this is to split your weekly dose and inject twice-weekly (every 3.5 days) which will clip the peak--->trough and blood levels will be more stable throughout the week.
Also keep in mind depending on the dose of T some men following a once weekly injection protocol may not hit a high enough trough TT/FT 7 days later whereas others may still be hitting a healthy/high trough FT.
Unfortunately your blood work was done at the wrong time as you always want to test at the true trough (lowest point) before your next injection.
Seeing as you are injecting once weekly then your true trough would be 7 days post-injection.
Your blood work was done 5 days post injection and your are hitting a high-end TT 873 ng/dL which means your peak would easily be over 1000 ng/dL.
The shitkicker here is not only did you have your blood work done at the wrong time but you are missing one of the most important blood markers free testosterone.
Although TT is important to know FT is what truly matters as it is the active unbound fraction of T responsible for the positive effect.
Bottomline here is TT means nothing without knowing where your FT level sits.
Even then if you are hitting a very high TT almost 900 ng/dL 5 days post-injection you would still be hitting a descent true trough TT (7 days) post-injection.
One could still end up hitting a healthy trough FT with a trough TT 700 ng/dL.
Again this means nothing without knowing where your FT and SHBG sit.
4. I've decided to do 50mg every 3.5 days to see if it helps. What will that do to my testosterone numbers? Will I still get up to around 1000 doing it that way or will it keep me lower but without the peaks and valleys?
Would not get to caught up on this needing to hit a TT 1000s especially if you are talking trough here!
One can easily hit a healthy/high trough FT with a trough TT <1000 ng/dL.
Again where your FT sits is what truly matters.
If you already jumped the gun and are going to switch over to injecting twice-weekly then you will need to start over again and wait 4-6 weeks for blood levels to stabilize before getting blood work done let alone a more thorough set of labs which will include your trough FT let alone other blood markers such as SHBG, DHT, prolactin and CBC.
Top it all off that every protocol needs to be given a fighting chance 12 weeks to claim whether it was truly as success or failure.
As I have preached numerous times on the forum over the years whether starting TTh or tweaking a protocol (increasing/decreasing T dose) hormone will be in FLUX during the weeks leading up until blood levels have stabilized (4-6 weeks TC/TE) and it is common for most to experience ups/downs during the transition as the body is trying to ADJUST.
Even then once blood levels have stabilized (4-6 weeks TC/TE) it will still take time as in a few more months for the body to ADAPT to its new set-point and this is the critical time period when one needs to gauge how they truly feel overall regarding relief/improvement of low-t symptoms and overall well-being.
Most do not understand how exogenous T works and start tweaking their protocols 6 weeks in because they do not feel good!
5. I am not on any kind of blockers because he didn't see any harmful side effects yet. Is the estradiol a concern at those numbers?
Tread lightly when it comes to use of an AI let alone the need for one!
Ts metabolites estradiol and DHT are needed.
Having healthy levels of estradiol is critical!
Ts metabolites estradiol and DHT are needed in healthy amounts to experience the full spectrum of testosterones beneficial effects on
(cardiovascular health, brain health, libido, erectile function, bone health, tendon health, immune system, lipids, and body composition).