FunkOdyssey
Seeker of Wisdom
His forum presence died, not the man himself.Readalot died????
His forum presence died, not the man himself.Readalot died????
Ohhhh, ok. Thanks for clarifying.His forum presence died, not the man himself.
I was told by my doctor the further out from the donation, the more accurate the lab test. The blood donation center said the same thing.so the tldr is keep it under 54? im reading that donating doesnt do much since it returns to high baseline within weeks plus it tanks ferritin.
I had no symptoms either at 59% but when the machine taking my blood shut down, I got kind of freaked out. I certainly agree with the 54% cut off. After that it time to start doing something about it.Comorbidities is what causes harm, not so much the hematocrit value.
I once had an HCT at 57% and my endo was advised to do nothing unless I had specific symptoms.
Things are starting to change, one doctor at a time.
Not true at all here is a RECENT quote from Morgentaler "in many ways the hematocrit and erythrocytosis is one of the most problematic issues in clinical use of testosterone therapy. It's a problem not necessarily because we see problems with it but because everybody believes it is a problem. Elevated hematocrit or hemoglobin in a naturally occurring population is not the same as testosterone related increases. Who has naturally occurring elevated hematocrit? Well it's patients that have other conditions COPD, sleep apnea, polycythemia vera. Those are not the same. I think we need to be careful about saying that they are the same. 9.999% of people that have strokes around the world are not on testosterone. So you can have a hematocrit of anything, you can be anemic, and have a stroke. So the hematocrit may have been contributory or it just may have been a random thing. But the point is all the randomized control trials that we have strokes and thrombotic events are extremely low.The person that wrote for the endocrine guidelines on testosterone therapy and who wrote the hematocrit section was Glenn Cunningham. I asked him both on stage and in person where did you come up with 54%? His answer was we actually don't have much data to say anything but we had to pick a number and it seemed like a reasonable number. The point is is that it's not really based on medical data. The reason we have to keep the hematocrit below 54% is because if something happens there is some vulnerability because of what the guidelines say. " Abraham Morgentaler April 13th 2023.This is ridiculous.
54% is considered the cutoff and the top guns in the field such as Dr. Morgentaler, Khera, Ramasamy, and many others preach this!
Madman you are a master at promoting your opinions and most of your opinions are not based on actual medical data. You bully men on the forum based on your opinions and most are in fact rubbish. Especially your opinions based on levels. Normal physiologic levels when on testosterone is not based on any medical data. Let me repeat that they are opinions based on the authors of the guidelines and not based on any medical literature that shows that when testosterone therapy is provided to a man that one should aim at a very specific number like the mid normal range for instance. And let me bust your bubble a little more and tell you that there is no medical literature to support maintaining a man's testosterone levels within the normal physiologic range when on testosterone therapy. You suffer from extreme belief perseverance and confirmation bias.Go push that shit on bumnation!
So you're OK with a free test double the top of the reference range and a hct of >60?Madman you are a master at promoting your opinions and most of your opinions are not based on actual medical data. You bully men on the forum based on your opinions and most are in fact rubbish. Especially your opinions based on levels. Normal physiologic levels when on testosterone is not based on any medical data. Let me repeat that they are opinions based on the authors of the guidelines and not based on any medical literature that shows that when testosterone therapy is provided to a man that one should aim at a very specific number like the mid normal range for instance. And let me bust your bubble a little more and tell you that there is no medical literature to support maintaining a man's testosterone levels within the normal physiologic range when on testosterone therapy. You suffer from extreme belief perseverance and confirmation bias.
Not true at all here is a RECENT quote from Morgentaler "in many ways the hematocrit and erythrocytosis is one of the most problematic issues in clinical use of testosterone therapy. It's a problem not necessarily because we see problems with it but because everybody believes it is a problem. Elevated hematocrit or hemoglobin in a naturally occurring population is not the same as testosterone related increases. Who has naturally occurring elevated hematocrit? Well it's patients that have other conditions COPD, sleep apnea, polycythemia vera. Those are not the same. I think we need to be careful about saying that they are the same. 9.999% of people that have strokes around the world are not on testosterone. So you can have a hematocrit of anything, you can be anemic, and have a stroke. So the hematocrit may have been contributory or it just may have been a random thing. But the point is all the randomized control trials that we have strokes and thrombotic events are extremely low.The person that wrote for the endocrine guidelines on testosterone therapy and who wrote the hematocrit section was Glenn Cunningham. I asked him both on stage and in person where did you come up with 54%? His answer was we actually don't have much data to say anything but we had to pick a number and it seemed like a reasonable number. The point is is that it's not really based on medical data. The reason we have to keep the hematocrit below 54% is because if something happens there is some vulnerability because of what the guidelines say. " Abraham Morgentaler April 13th 2023.
When Ramasamy was asked directly does he think the elevator hematocrit causes harm his response was "no "but what I'm looking at now is there a potential harm based on the magnitude of change in hematocrit when one starts testosterone
So madman this fear that you perpetrate it's not based on any medical data at all in men on testosterone therapy. Are you now going to state that everyone that lives above 2500 m that has an elevated hematocrit is at risk? That's exactly what you're saying if you're saying that the elevator hematocrit on testosterone increases a man's risk.
What is happening presently is what happened with testosterone and prostate cancer. It was thought to cause prostate cancer for over seven decades and now we know it is the opposite. We are seeing the same with the elevated hematocrit. The fear of testosterone causing prostate cancer was not based on any medical data but yet it was still widely believed and it still is. The same holds true for the elevated hematocrit while on testosterone. I keep saying while on testosterone. Not baseline elevation.
Testosterone Therapy as a cause of Secondary Erythrocytosis
The most common side effect of testosterone therapy, and the one that causes the most concern for the patient and their family physician, is a secondary erythrocytosis which is an increase in red blood cells. It is often described by the patient and their physician as “thick blood” requiring a blood donation because they fear it could possibly lead to a heart attack, stroke, or blood clot. Where does this fear originate? When the family physician or internist sees an increase in red blood cells along with hemoglobin and hematocrit, it is frequently misinterpreted as the patient having Polycythemia Vera which is a myeloproliferative neoplasm of the bone marrow (bone marrow cancer). Thrombosis (blood clots) are a leading cause of morbidity and mortality in this disorder. Polycythemia vera is known as a primary erythrocytosis where there is an unregulated proliferation of hematopoietic clonal stem cells which leads to over production of red blood cells, white blood cells, and platelets. In Polycythemia Vera, in contrast to the secondary erythrocytosis from testosterone therapy, not only is there a quantitative change in the number of circulating blood cells, but there is also a qualitative change that leads to the expression of procoagulant characteristics. In addition there are abnormalities involving the vascular endothelial cells which become procoagulant in response to inflammatory stimuli. These abnormalities result in a hypercoagulable state leading to an
increase in arterial thrombosis and venous thrombosis. Therefore part of the recommended treatment is blood donation to reduce the risk of thrombosis. The risk of elevated hematocrit seen in patients with polycythemia vera cannot be extrapolated to hematocrit elevation seen during testosterone therapy. They are not the same and should not be treated as such.
The secondary erythrocytosis from testosterone therapy is an increase in red blood cells only leading to an increase in hemoglobin and hematocrit. The mechanisms behind testosterone stimulating red blood cell production is not completely understood but is thought to occur through stimulation of erythropoietin, stimulation of hematopoietic progenitor cells, and reduced hepcidin. A secondary erythrocytosis is also seen in other conditions such as smoking, obstructive sleep apnea, chronic obstructive pulmonary disease, and living at high altitude. While a primary erythrocytosis has been well established as a risk factor for thromboembolic events the secondary erythrocytosis from testosterone therapy has not been shown to cause an increase in thromboembolic events in any randomized control trial or prospective study to date.
The other concern with increasing hematocrit is that it will increase viscosity and decrease blood flow resulting in thrombotic events. In experimental studies using rigid glass viscometers or cone-plate viscometers there is a logarithmic increase in viscosity
with increasing hematocrit. It is inappropriate to correlate these in vitro viscosity readings to what occurs to flowing blood through tiny distensible vessels in vivo. In other words, viscometer measures in these experiments do not translate to human blood vessels. Firstly, the flow through these narrow blood vessels is rapid (high shear rate), which in a non-Newtonian fluid such as blood causes a marked decrease in viscosity. Second, blood flowing through these narrow channels is axial with a central core of packed red blood cells sliding over a peripheral layer of lubricating low viscosity plasma. With a secondary erythrocytosis there is an increase in blood volume which enlarges the vascular bed, decreases peripheral resistance and increases cardiac output. Therefore, in a secondary erythrocytosis optimal oxygen transport with increased blood volume occurs at a higher hematocrit value than with a normal blood volume. A moderate increase in hematocrit may be beneficial despite the increased viscosity.
Currently, numerous testosterone formulations are available, including short and long-acting injections, topical gels, topical creams, implantable pellets, transdermal and buccal patches, oral testosterone , and nasal sprays. All types of testosterone therapies result in a statistically significant increase in hematocrit when compared to placebo and this increase is more pronounced in older than younger men. These increases in hematocrit are both dose dependent and serum level dependent. Short acting
testosterone injections have been associated with a greater incidence of increased hematocrit compared with other methods of delivery in multiple studies. These studies did not include any compounded products such as the compounded testosterone cream that is available in concentrations up to 200 mg/ gram in various delivery bases. This 20% concentration is much higher than the commercially available topical testosterone creams or gels. The serum levels of testosterone obtained with these compounded products are similar to that obtained with the short acting injectable testosterone preparations , therefore, the incidence of increased hematocrit may not differ significantly between these two methods of delivery.
Guidelines vary depending on the country and the medical society with regard to the upper limit of normal for hematocrit in men on testosterone therapy. The Canadian guidelines cite a hematocrit of 55% as the safe upper limit, while the European Association of urology, the American Urology Association, and the Endocrine society state that the hematocrit should not exceed 54%. Most guidelines recommend following hematocrit after initiating testosterone therapy and if the Hct exceeds 54% clinicians should either adjust testosterone dosage, stop therapy, order phlebotomy, or recommend a combination of these. These recommendations are based on assumptions and the Hct cut off of 54% was arbitrarily chosen and not based on any study showing harm when this value is exceeded with testosterone
therapy. In fact, when Dr. Glenn Cunningham one of the authors of the Endocrine Society's guidelines for testosterone therapy was asked by Dr. Abraham Morgentaler where the upper limit of 54% came from he replied that “the number was not based on any actual medical data ,but we had to pick a number and it seemed like a reasonable number”. The upper limit of normal for hematocrit in most laboratory reference ranges for healthy adult males is 54% which is where this value is likely derived. Also creating confusion is the fact that different labs have different upper limits of normal for hematocrit. Some may use an upper limit of normal of 50% and others 54%. If you are a midshipmen on the USS Eisenhower, one of our nuclear aircraft carriers, the upper limit of normal for hematocrit in their lab is 60% (image 1)
These normal ranges of hematocrit are for men without a secondary erythrocytosis and not for men on testosterone or living at high altitude for instance. There are over 80 million people that live higher than 2,500 meters and they develop a secondary erythrocytosis. Men in parts of Bolivia for instance have a normal range of Hct from 45-61%. These men are not at an increased risk of thrombotic events nor do they have to undergo phlebotomies to manage their hematocrit. One also cannot ignore the observation that literally tens of thousands of men presently use and abuse testosterone in this country and have done so for decades. A large percentage of these men are not under the supervision of a physician or getting lab work and yet we have not
seen an epidemic of heart attacks, strokes, or blood clots in these men. Almost all previously reported cases of testosterone therapy related venous thromboembolism were seen in patients with a previously undiagnosed thrombophilia like factor five Leiden deficiency.
Testosterone also exerts multiple beneficial effects on the vasculature and its components which may protect against thrombosis. In other words testosterone has positive effects on vascular reactivity .Testosterone is a vasodilator and increases nitric oxide. Testosterone decreases plasma concentrations of pro coagulatory substances and reduces levels of lipoprotein a. Testosterone increases red blood cell deformability and improves erythrocyte membrane lipid composition and fluidity.
The donation of blood for altruistic reasons is both necessary and commendable. It is imperative that we maintain our blood supply as every two seconds someone in the United States needs blood or platelets. Every day, whole blood donations help save the lives of children and adults fighting to survive cancer, blood disorders, traumatic injuries and more. The American red cross allows whole blood donation as often as every 56 days up to six times a year. Several positive effects of blood donation have been described in the medical literature including feelings of satisfaction, greater alertness, and increased well-being etc. Minor adverse effects such as fatigue, vasovagal symptoms,
fainting and bruising can occur in some individuals. The main concern is the development of Iron deficiency anemia which can occur in up to 35% of repeat donors. Moderately trained athletes may also see a decrement in performance after whole blood donation. Maximal power output, VO2 max, and hemoglobin mass were decreased up to four weeks after a single whole blood donation in moderately trained people. Beneficial training adaptations were also lowered by repeated whole blood donations. Some athletes may want to consider plasma donation as an alternative as it will not have an effect on their hemoglobin levels.
Many asymptomatic men on testosterone donate blood out of fear and not altruism. This fear is propagated by clinics even though no randomized or prospective studies have observed a direct relation between the testosterone induced secondary erythrocytosis and thromboembolic events. Some men will report that they feel better after a blood donation and that can be secondary to several factors in addition to what has been previously discussed. Firstly, blood donation elicits an adrenal response. Secondly, blood donation will decrease the anxiety and fear associated with the increase in hematocrit . Because of repeated, and at times unnecessary donations, men unknowingly develop an Iron deficiency anemia and the associated symptoms of fatigue, weakness, shortness of breath, exercise intolerance, and rapid heart rate etc. In many instances these symptoms will be
wrongly blamed on testosterone or one of its active metabolites such as DHT or estradiol leading to unnecessary adjustments in dosages and levels. Donating blood to reduce hematocrit may also provide men with a false sense of security. In a study done over a two-year period of time they looked at men who donated blood that were on testosterone therapy and at least 25% of them had a hematocrit above 54% and when they came back for repeat donations 44% of them had a persistent elevation of hematocrit above 54%. So it essentially showed that repeat donations were insufficient to maintain a hematocrit below 54% in many men.
In contrast to asymptomatic otherwise healthy men on testosterone, men on testosterone therapy with unknown or known comorbid conditions such a sleep apnea, obesity, type II diabetes etc..that develop symptoms they attribute to increased hematocrit such as headache, dizziness, shortness of breath, or fatigue etc...can donate blood and either stop therapy or adjust dosage to control symptoms. Men who develop an excessive erythrocytosis during testosterone therapy should also be evaluated for sleep apnea, and if diagnosed should undergo appropriate treatment so as to better tolerate a therapeutic dose of testosterone. Testosterone therapy should be based on clinical effect and therapeutic response while avoiding unwanted side effects.
Testosterone therapy was first used clinically in the mid 1930’s and it has been used in thousands of randomized control trials. There is not a single randomized control trial to date that shows an increased risk of major adverse cardiac events with testosterone therapy.
We really don’t see anyone with a hematocrit of 60 and if they do, it’s usually because they have concomitant sleep apnea and once they get that treated it comes right down. Mine is 57.8 if that answers your question. And yes myself and every single person that has it is very happy. With a free testosterone. Double the top of the reference range. In fact, some men have a free testosterone triple the reference range. By you asking that question you do not understand where the reference range comes from. You want to read the article that is attached by Dr. Rebecca Glasser even treating females where they have levels 4 to 6 times the normal physiologic range for females and everything improves without any adverse events. Same thing happens with males. You also don’t understand what’s happening with the so-called normal range as it has been dropping for decades. It coincides And parallels the increase in industrial chemicals. Men’s sperm counts have also dropped by 50%. They go hand-in-hand as you have to have adequate intra testicular testosterone levels for normal spermatogenesis. The new normal range was changed in July 2017 and it used to go up to almost 1200 and now it goes up to 916. So are you telling me that a normal level of 1100 in June 2017 is all of a sudden dangerous and abusive After July 2017? It is now supra physiologic, but then it was completely normal. You may have been brainwashed by the word super physiologic, and it has been hijacked to mean abuse and harm and it is never caused harm. We’re not talking about the bodybuilding world either. But a free testosterone of 30 to 60 and a man that needs it is perfectly fine and in fact, healthy, and every parameter of health improves that you can measure in these men. But everyone’s entitled to keep their testosterone levels as low as they want. But the problem is is men like mad men having an opinion otherwise which is not based on any medical data. There is no medical data to support the guidelines stating we should aim for the mid normal range. No studies at all. It’s just an opinion and there are no studies or medical data that supports the opinion that testosterone remit should remain within the normal physiologic range on treatment. It once again is an opinion not based on medical fact. When you’re treating man, most all men get better with levels outside of the normal range, which goes up to 917 right now for instance. Not every man needs that but what we’re all saying is that men should not be deprived that do need it. Everyone can keep their levels as low as they want but for various reasons higher levels. I don’t have two hours to explain this to you, but I’ll leave it at that but you can watch some videos coming up where it is explained.So you're OK with a free test double the top of the reference range and a hct of >60?
Didn’t you just babble that the leaders in the field made the cut off at 54% ? I pointed out to you that Morgentaler has changed his stance and Mel knows that a Hct above 54% is not harmful while on testosterone. You also bully and degrade men for having testosterone levels outside of the normal sick range. Yes, madman men need testosterone , and they need their levels to be super physiologic most of the time. The upper cut off is 917 now so 918 is now super physiologic. You have a strong opinion on numbers. Let me give you an example if you were a physician. A patient comes to see you and he needs testosterone so you give it to him at your normal starting dose. His levels come back at 700 let’s say and a free 18 and he says I’m still having a lot of problems with erectile dysfunction and fatigue and depression and I’m continuing to gain weight and lose muscle despite exercising and dieting, etc. So mad man hopefully will increase the dose And then he comes back with a level of 1500 and he says man I feel great. All my symptoms have completely resolved. My lipids have improved, I’ve lost 30 pounds, I no longer have any erectile dysfunction, I don’t have any fatigue, and I feel great. I’m off of my statin and I don’t take blood pressure medicines anymore. My free testosterone is 50 by the way. Mad man then says “no man needs a free testosterone of 50 you need to lower your dose “so he lowers his dose and then he goes back to feeling bad and comes back and says I don’t feel good mad man And mad man will say too bad because you don’t need the level that you had before. Madman treats, a number not a patient. You have repeatedly done this over and over again the men on this forum where you attacked them for their levels yet they’re doing fine with their levels, and every parameter of their health are improving. You need to get your head out of where the sun doesn’t shine.You should very well know that most of the shit you are constantly babbling about on here has been posted by me on the forum in numerous threads!
Where on the forum did I ever state that running a hematocrit >54% was dangerous or that it is a given someone will be more prone to negative effects on cardiovascular health?
Madman you are a master at promoting your opinions and most of your opinions are not based on actual medical data. You bully men on the forum based on your opinions and most are in fact rubbish. Especially your opinions based on levels. Normal physiologic levels when on testosterone is not based on any medical data. Let me repeat that they are opinions based on the authors of the guidelines and not based on any medical literature that shows that when testosterone therapy is provided to a man that one should aim at a very specific number like the mid normal range for instance. And let me bust your bubble a little more and tell you that there is no medical literature to support maintaining a man's testosterone levels within the normal physiologic range when on testosterone therapy. You suffer from extreme belief perseverance and confirmation bias.
But hey brother, you realize the hematocrit is 60% is normal in some labs don’t you? It’s normal on our nuclear aircraft carriers. It’s normal if you live at high altitude in certain areas of the world. Why are they not all dropping dead a heart attack strokes and blood clots? Can you answer me that?So you're OK with a free test double the top of the reference range and a hct of >60?
Here you go babbling about the normal physiologic range again. Let me let you in on some new insights since you’re behind the curve. Aiming for a normal physiologic number is not based on medical data. Have you ever taken the time to think that maybe when we take testosterone it acts differently than we make it ourselves. There are a lot of complex physiological events that occur when we make testosterone ourselves and if we can make a level of 700, 800, 900 even 1000 ourselves we would all probably be fine. It’s more than just testosterone, because there are many physiological events that occur when you make it naturally, and we bypass all of that when we take testosterone. When we just get the end product, men need a dose that takes them out of the physiologic range to get the same response then if we make it ourselves. many physicians are realizing this now because we have seen that clinically now for decades. Dozens of studies show that testosterone doesn’t work and in all of those studies, they only raise testosterone to the mid physiologic range and being didn’t get better. The normal range is not a healthy range because men’s testosterone levels have been dropping for decades. The new normal range, and the new physiologic range that you referred to is deficient. The new normal is to be deficient. when you treat actual people and that numbers, you will see that most all of them need a number outside of the normal physiologic range to resolve symptoms and every parameter of their health improves. You don’t know this because you don’t see this.LMFAO!
Never had an issue with someone running levels and yes that would be trough levels beyond the top end of the physiological range within reason if overall blood markers are healthy and they feel great.
Never promoted let alone told anyone on the forum that their levels need to stay within a set reference range.
Yes, we have a few members who may be sticklers but I am not one of them.
A big difference between running healthy/high-end trough levels vs absurdly high trough levels.
Just to be clear keep my name out of your piehole!
You ran it off on one of your channels back when I first came on Excel.
And something else that you’re obviously unaware of madman, is that the normal range for free test Strong is internally derived from LabCorp and quest, and we know nothing about those men, especially with regard to their health status, hormone status, or symptomatology. They came up with the numbers themselves. So you’re wanting men to be confined to a free testosterone level that nobody has any idea that they came up with because they didn’t publish it. When you look at recent studies done in 2020 where they did evaluate free testosterone levels in men. The free testosterone levels were double what quest has as a normal level. You have a lot to learn and you need to keep your opinion to a minimum and open yourself up to new ideas and ask questions about why we all do what we do and most of the time the answer is just because they did it before and nobody ever asked the question why. Why do we aim for the normal mid physiologic range? Where did that come from? It was an opinion .LMFAO!
Never had an issue with someone running levels and yes that would be trough levels beyond the top end of the physiological range within reason if overall blood markers are healthy and they feel great.
Never promoted let alone told anyone on the forum that their levels need to stay within a set reference range.
Yes, we have a few members who may be sticklers but I am not one of them.
A big difference between running healthy/high-end trough levels vs absurdly high trough levels.
Just to be clear keep my name out of your piehole!
You ran it off on one of your channels back when I first came on Excel.
Didn’t you just babble that the leaders in the field made the cut off at 54% ? I pointed out to you that Morgentaler has changed his stance and Mel knows that a Hct above 54% is not harmful while on testosterone. You also bully and degrade men for having testosterone levels outside of the normal sick range. Yes, madman men need testosterone , and they need their levels to be super physiologic most of the time. The upper cut off is 917 now so 918 is now super physiologic. You have a strong opinion on numbers. Let me give you an example if you were a physician. A patient comes to see you and he needs testosterone so you give it to him at your normal starting dose. His levels come back at 700 let’s say and a free 18 and he says I’m still having a lot of problems with erectile dysfunction and fatigue and depression and I’m continuing to gain weight and lose muscle despite exercising and dieting, etc. So mad man hopefully will increase the dose And then he comes back with a level of 1500 and he says man I feel great. All my symptoms have completely resolved. My lipids have improved, I’ve lost 30 pounds, I no longer have any erectile dysfunction, I don’t have any fatigue, and I feel great. I’m off of my statin and I don’t take blood pressure medicines anymore. My free testosterone is 50 by the way. Mad man then says “no man needs a free testosterone of 50 you need to lower your dose “so he lowers his dose and then he goes back to feeling bad and comes back and says I don’t feel good mad man And mad man will say too bad because you don’t need the level that you had before. Madman treats, a number not a patient. You have repeatedly done this over and over again the men on this forum where you attacked them for their levels yet they’re doing fine with their levels, and every parameter of their health are improving. You need to get your head out of where the sun doesn’t shine.
Didn’t you just babble that the leaders in the field made the cut off at 54% ? I pointed out to you that Morgentaler has changed his stance and Mel knows that a Hct above 54% is not harmful while on testosterone.

You obviously post but don't really read anything that you post including the literature. I just sent you a quote from Abraham Morgenthaler that I have actually tape recorded. It is from April of this year he has changed his stance or did you not catch that with my previous explanation. You should probably read and learn something from time to time instead of immediately thinking about what you wanna say without processing what you could have read. Morgentaler adamantly states now that the hematocrit of 54% on testosterone is not harmful even if going above it. It's only harmful because of what other physicians don't know about it. Those are exact quotes from him, so what do you not get that I'm telling you? You're posting an old lecture. Get with the times the updated times. And what is your definition of absurdly high levels? That's your opinion not based on any clinical observations are any actual treatment of men yourself. You have zero clinical experience. It's your opinion. And let me ask you this. Why does anybody have to have a trough? Do you even know why they test at trough? Doctors were taught to do that because they didn't want to see the levels at peak because it would scare them. Depending on the dose whether it be one or 200 mg of testosterone cypionate some mens levels will be anywhere from 2 to 4000.Again who stated it is harmful?
From my previous reply in post #6.
Yes, this is recent!
Lets get Abe on here?
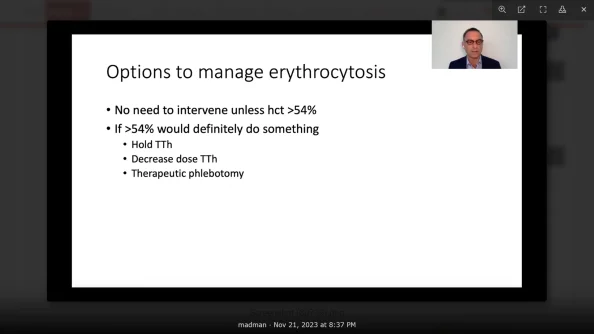
This sums it up and this is coming from one who would be considered the father of testosterone!
This is f**KING GOLD!
* No need to intervene unless hct>54%
* If >54% would definitely do something
View attachment 39364
You also bully and degrade men for having testosterone levels outside of the normal sick range. Yes, madman men need testosterone , and they need their levels to be super physiologic most of the time. The upper cut off is 917 now so 918 is now super physiologic. You have a strong opinion on numbers.
Already burned you on that one in my previous reply!
Did you forget that I run a high trough FT?
Mad man then says “no man needs a free testosterone of 50 you need to lower your dose “so he lowers his dose and then he goes back to feeling bad and comes back and says I don’t feel good mad man And mad man will say too bad because you don’t need the level that you had before. Madman treats, a number not a patient. You have repeatedly done this over and over again the men on this forum where you attacked them for their levels yet they’re doing fine with their levels, and every parameter of their health are improving. You need to get your head out of where the sun doesn’t shine.
Slow in the head I see or better yet putting words in people's mouths.
Never once have I told anyone who was running a high trough FT level that felt great overall let alone blood markers were healthy to change their protocol.
Again big difference between someone running a high-end/high trough FT level vs. absurdly high levels.
You obviously post but don't really read anything that you post including the literature. I just sent you a quote from Abraham Morgenthaler that I have actually tape recorded. It is from April of this year he has changed his stance or did you not catch that with my previous explanation. You should probably read and learn something from time to time instead of immediately thinking about what you wanna say without processing what you could have read. Morgentaler adamantly states now that the hematocrit of 54% on testosterone is not harmful even if going above it. It's only harmful because of what other physicians don't know about it. Those are exact quotes from him, so what do you not get that I'm telling you? You're posting an old lecture. Get with the times the updated times. And what is your definition of absurdly high levels? That's your opinion not based on any clinical observations are any actual treatment of men yourself. You have zero clinical experience. It's your opinion. And let me ask you this. Why does anybody have to have a trough? Do you even know why they test at trough? Doctors were taught to do that because they didn't want to see the levels at peak because it would scare them. Depending on the dose whether it be one or 200 mg of testosterone cypionate some mens levels will be anywhere from 2 to 4000.
And the father of testosterone. Well, I know him personally and I talked to him personally regarding the hematocrit issue this year. So get rid of the old information and come on in with the new.
So you don't understand what he's doing with that slide presentation do you? He understands and knows there's no harm with raising the hematocrit above 54% when men are on testosterone as he has stated publicly. I will be glad to send you the recording of him at the androgen society. The reason he makes these recommendations on the slides is to prevent other physicians from getting in trouble by their colleagues that don't know any better. So the point is he knows there's no harm but we all still use that 54% to protect ourselves from our colleagues. He pointed this out very specifically. It doesn't cause harm he said, but others don't know that and that could cause you harm if something happens to the patient because they're going to blame it on you even though we know it doesn't cause harm. Let that sink in a little bit madman because you're just not privy to the inside information.
And now that I've had the opportunity to view your post over the years now it's become very evident that you can post some very good articles, but that you don't read and process any of them.Again who stated it is harmful?
From my previous reply in post #6.
Yes, this is recent!
Lets get Abe on here?
This sums it up and this is coming from one who would be considered the father of testosterone!
This is f**KING GOLD!
* No need to intervene unless hct>54%
* If >54% would definitely do something
View attachment 39364
You also bully and degrade men for having testosterone levels outside of the normal sick range. Yes, madman men need testosterone , and they need their levels to be super physiologic most of the time. The upper cut off is 917 now so 918 is now super physiologic. You have a strong opinion on numbers.
Already burned you on that one in my previous reply!
Did you forget that I run a high trough FT?
Mad man then says “no man needs a free testosterone of 50 you need to lower your dose “so he lowers his dose and then he goes back to feeling bad and comes back and says I don’t feel good mad man And mad man will say too bad because you don’t need the level that you had before. Madman treats, a number not a patient. You have repeatedly done this over and over again the men on this forum where you attacked them for their levels yet they’re doing fine with their levels, and every parameter of their health are improving. You need to get your head out of where the sun doesn’t shine.
Slow in the head I see or better yet putting words in people's mouths.
Never once have I told anyone who was running a high trough FT level that felt great overall let alone blood markers were healthy to change their protocol.
Again big difference between someone running a high-end/high trough FT level vs. absurdly high levels.
I'm sure you have a great response, but wall of text is a bit too much.We really don’t see anyone with a hematocrit of 60 and if they do, it’s usually because they have concomitant sleep apnea and once they get that treated it comes right down. Mine is 57.8 if that answers your question. And yes myself and every single person that has it is very happy. With a free testosterone. Double the top of the reference range. In fact, some men have a free testosterone triple the reference range. By you asking that question you do not understand where the reference range comes from. You want to read the article that is attached by Dr. Rebecca Glasser even treating females where they have levels 4 to 6 times the normal physiologic range for females and everything improves without any adverse events. Same thing happens with males. You also don’t understand what’s happening with the so-called normal range as it has been dropping for decades. It coincides And parallels the increase in industrial chemicals. Men’s sperm counts have also dropped by 50%. They go hand-in-hand as you have to have adequate intra testicular testosterone levels for normal spermatogenesis. The new normal range was changed in July 2017 and it used to go up to almost 1200 and now it goes up to 916. So are you telling me that a normal level of 1100 in June 2017 is all of a sudden dangerous and abusive After July 2017? It is now supra physiologic, but then it was completely normal. You may have been brainwashed by the word super physiologic, and it has been hijacked to mean abuse and harm and it is never caused harm. We’re not talking about the bodybuilding world either. But a free testosterone of 30 to 60 and a man that needs it is perfectly fine and in fact, healthy, and every parameter of health improves that you can measure in these men. But everyone’s entitled to keep their testosterone levels as low as they want. But the problem is is men like mad men having an opinion otherwise which is not based on any medical data. There is no medical data to support the guidelines stating we should aim for the mid normal range. No studies at all. It’s just an opinion and there are no studies or medical data that supports the opinion that testosterone remit should remain within the normal physiologic range on treatment. It once again is an opinion not based on medical fact. When you’re treating man, most all men get better with levels outside of the normal range, which goes up to 917 right now for instance. Not every man needs that but what we’re all saying is that men should not be deprived that do need it. Everyone can keep their levels as low as they want but for various reasons higher levels. I don’t have two hours to explain this to you, but I’ll leave it at that but you can watch some videos coming up where it is explained.
And something else that you’re obviously unaware of madman, is that the normal range for free test Strong is internally derived from LabCorp and quest, and we know nothing about those men, especially with regard to their health status, hormone status, or symptomatology. They came up with the numbers themselves. So you’re wanting men to be confined to a free testosterone level that nobody has any idea that they came up with because they didn’t publish it. When you look at recent studies done in 2020 where they did evaluate free testosterone levels in men. The free testosterone levels were double what quest has as a normal level. You have a lot to learn and you need to keep your opinion to a minimum and open yourself up to new ideas and ask questions about why we all do what we do and most of the time the answer is just because they did it before and nobody ever asked the question why. Why do we aim for the normal mid physiologic range? Where did that come from? It was an opinion .
 www.labcorp.com
www.labcorp.com
Get the latest men's health insights, expert advice, and community updates delivered to your inbox.