
Seagal
Well-Known Member
Identification of a leucine-mediated threshold effect governing macrophage mTOR signalling and cardiovascular risk - Nature Metabolism
Zhang et al. use human studies and mechanistic work in mouse models to describe how leucine serves as the key amino acid derived from dietary protein to drive deleterious macrophage mTORC1 signalling and promote cardiovascular disease.
 www.nature.com
www.nature.com
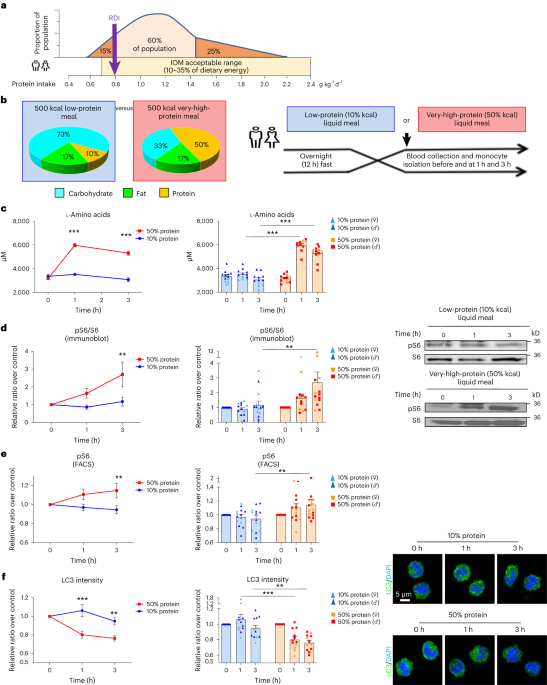
High protein intake is common in western societies and is often promoted as part of a healthy lifestyle; however, amino-acid-mediated mammalian target of rapamycin (mTOR) signalling in macrophages has been implicated in the pathogenesis of ischaemic cardiovascular disease. In a series of clinical studies on male and female participants (NCT03946774 and NCT03994367) that involved graded amounts of protein ingestion together with detailed plasma amino acid analysis and human monocyte/macrophage experiments, we identify leucine as the key activator of mTOR signalling in macrophages. We describe a threshold effect of high protein intake and circulating leucine on monocytes/macrophages wherein only protein in excess of ∼25 g per meal induces mTOR activation and functional effects. By designing specific diets modified in protein and leucine content representative of the intake in the general population, we confirm this threshold effect in mouse models and find ingestion of protein in excess of ∼22% of dietary energy requirements drives atherosclerosis in male mice. These data demonstrate a mechanistic basis for the adverse impact of excessive dietary protein on cardiovascular risk.








