View attachment 56152
Took my first labs since starting TRT. Labs were drawn about 11 weeks since beginning a course of 120 Cyprionate split into two subq shots per week. Labs were taken at trough in the morning.
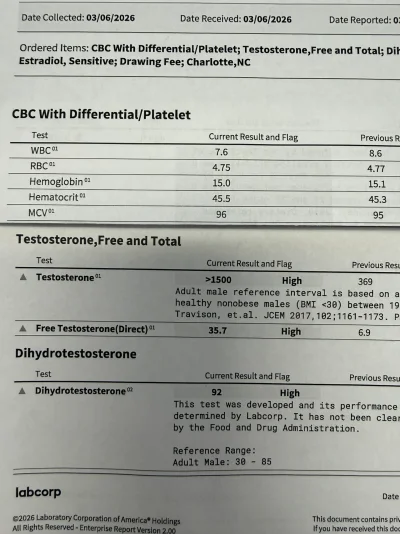
These latest labs (attached) seem nuts for the amount I’m taking?
- >1500 total
- 35.7 free,
- Estradiol 24.9
- DHT 92
Always post labs with the refernce ranges and testing methods used especially for the most critical fraction free testosterone.
Hard to believe no one pointed this out as your free testosterone was tested using a known to be inaccurate assay the direct IA which no one should be using/relying on.
The only way to know where your FT truly sits is to have it tested using the most accurate assay the gold standard Equilibrium Dialysis especially in cases of altered SHBG.
Otherwise you would need to use/rely on the next best testing method the go to calculated linear law-of-mass action Vermeulen (cFTV) which will give a good approximation.
The standard starting dose across the board by those in the know for the majority is 100 mg T/week or better yet 50 mg T split twice-weekly.
Yes many of the endos and some uros will start patients on 60-80 mg T/week but this is usually older men.
No one needs to be starting therapy >100 mg T/week as there will always be time to increase the dose if need be and some men can easily achieve a healthy/high trough FT injecting 100 mg T/week especially split twice-weekly.
Even then it is always best to start low and go slow on a T only protocol so we can see how your body reacts to T and where said protocol dose of T/injection frequency has your trough TT and more importantly FT, estradiol and SHBG let alone critical blood markers RBCs, hemoglobin and hematocrit.
Something is way off with your RBCs, hemoglobin and hematocrit as they barely budged and it is a given that you will see an increase when using androgens and driving up your trough/steady-state FT so chances are you have low iron/ferritin or some other underlying issue going on.
Most men on therapy are injecting 100-200 mg T/week whether once weekly or split into more frequent injections.
There will always be those outliers who may need the higher-end dose but its far from common as in rare.
Some men can achieve stellar levels injecting <100 mg T/week especially when split into more frequent injections.
The majority of men can easily hit a healthy/high trough FT injecting 100-150 mg T/week especially when split into more frequent injections.
Even 150 mg T/week can easily be overkill for many.
Keep in mind that although TT is important to know FT is what truly matters as it is the active unbound fraction of T responsible for the positive effects.
Too many still caught up on the TT when FT is where its at.
As you can see you were started on a slightly higher dose 120 mg T/week split 60 mg twice-weekly and you are hitting an absurd trough TT>1500 ng/dL 3.5 days post-injection.
Your TT was not even tested using the most accurate assay (LC-MS/MS) as it was tested using the direct IA which caps out at 1500 ng/dL so you have no idea where it truly sits.
Even more concerning is your FT was not tested using an accurate assay so we have no idea where it truly sits and we also have no clue where your SHBG sits as it was not tested but even then with an absurd trough TT >1500 ng/dL your trough FT would be high even if you had highish/high SHBG.
You had highish baseline SHBG before jumping on T so even if it never budged and chances are it may be lower from the androgen load if we calculate your FT using the go to cFTV with an absurd trough TT >1500 ng/dL, highish SHBG 39.5 nmol/L and Albumin 4.3 g/dL (default) then your trough FT would could easily be a whopping 37-40 ng/dL or much higher if your SHBG has decreased.
More importantly your peak TT, FT and estradiol will be
View attachment 56151
Even if a man had a high SHBG 60 nmol/L with a whopping trough TT >1500 ng/dL his trough FT would still be very high!
You would easily have room to lower your dose and bring down your trough FT if need be.
If anything I would retest your trough TT using the most accurate assay (LC-MS/MS) and your trough FT using the most accurate assay ED so you can see where they truly sit but again your trough FT is going to be high.
Definitely no need to increase your dose further this would be a disaster.
This is the panel you want when testing TT/FT as it uses the most accurate assays.

")













