

Hi Guys! Im new here, 35yr old male and pretty much tick off all the boxes of low test symptoms but just got my results back and I'm on the high side ( I do not know what kind of tests they ran), so my question to the experienced guys, whats next ? My doctor already told me regardless of the test results they wont help to optimize testosterone so I'm in this by myself (and this forum)
My results are:
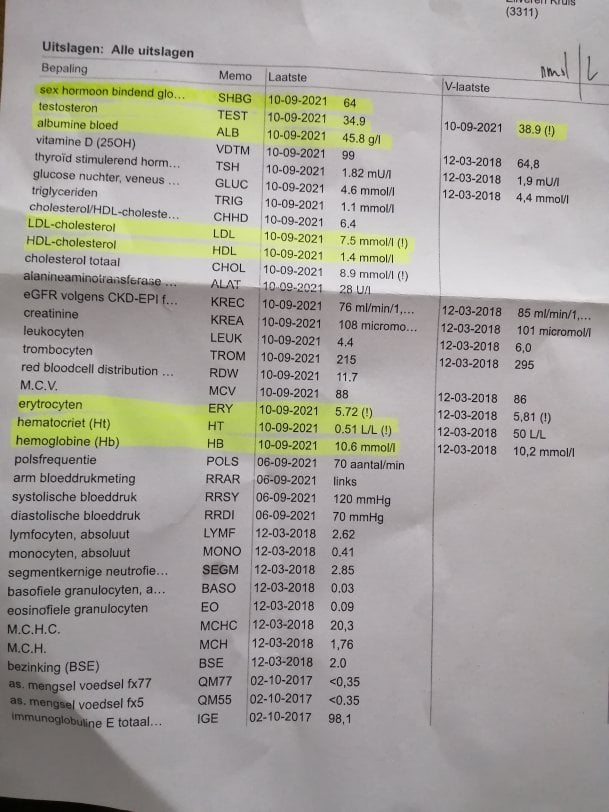
Testosterone 38.9 nmol/L - 1121.95 ng/dl
Albumin 45.8 g/L
SHBG 64nmol/L - 1845.88 ng/dl
Free Testosterone 0.526 nmol/L - 15.17 ng/dl - 1.51%
Bioavailable Testosterone 13.1 nmol/L - 377.83
I have used this website to calculate the free test, as my doctors lab didn't calculate it: Free & Bioavailable Testosterone calculator
Cheers,
Jack
My results are:
Testosterone 38.9 nmol/L - 1121.95 ng/dl
Albumin 45.8 g/L
SHBG 64nmol/L - 1845.88 ng/dl
Free Testosterone 0.526 nmol/L - 15.17 ng/dl - 1.51%
Bioavailable Testosterone 13.1 nmol/L - 377.83
I have used this website to calculate the free test, as my doctors lab didn't calculate it: Free & Bioavailable Testosterone calculator
Cheers,
Jack


 Dirk Lemke1*‡,
Dirk Lemke1*‡,  Rainer Johannes Klement
Rainer Johannes Klement









