In essence a "restart" is an attempt to restart the HPTA (hypothalamic-pituitary-testicular axis) for a patient who's axis is suppressed or shutdown due to being on TRT or AAS.
It is similar to a "stimulation" type regimen (as opposed to frank TRT), except for the starting point for a restart is typically a FULLY suppressed HPTA due to TRT/AAS, whereas the starting point for a general stimulation regimen is simply a sub-optimal or partially suppressed HPTA for various other factors (not current TRT/AAS use). Semantics really, the first paragraph gives the jist.
Hello Dr. Saya
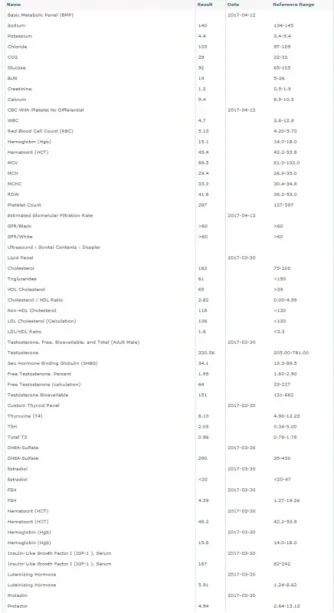
Is the restart protocol only for a patient who is suppressed/shutdown due to TRT/AAS? I currently have low T(330) and have been prescribed TRT(T + HCG). A lot of people told me to look into the HPTA restart protocol. Is that something recommended for a person who has never been on any AAS/TRT. Thank you for sharing your valuable inputs.
Last edited by a moderator: