Hi all.
I was diagnosed with hypogonadism when I was young (<20).
At first, I went to some horrible endos who prescribed me topical T cream when I was <20 years old! Fortunately, I only took this for a few months before I started reading and realizing this wasn't the way/that there were ways to preserve fertility by just making the pituitary do its job.
A better endo saw me and diagnosed me with type 2 hypo. He prescribed me with climid. I saw better test results then. But I stopped taking that too (I probably shouldn't have).
Things were going GREAT for awhile. I was working out, putting on 30 lbs of muscle, and I had zero issues for about 5 years...until now.
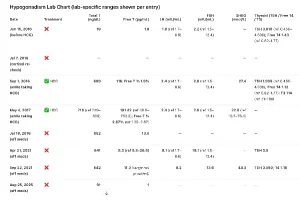
Over the last month or so, I noticed a libido drop. Got tested and the results were bad. You can see the chart I created attached.
Now I'm wondering if my type 2 has become type 1 or mixed. I guess when I re-test LH and FSH, I'll see.
Any thoughts you have would be appreciated. I'm going to push my doctor to get me the right bloodwork and to refer me to a good endo ASAP. Hopefully I don't need to wait 2 months for an appointment.
I was diagnosed with hypogonadism when I was young (<20).
At first, I went to some horrible endos who prescribed me topical T cream when I was <20 years old! Fortunately, I only took this for a few months before I started reading and realizing this wasn't the way/that there were ways to preserve fertility by just making the pituitary do its job.
A better endo saw me and diagnosed me with type 2 hypo. He prescribed me with climid. I saw better test results then. But I stopped taking that too (I probably shouldn't have).
Things were going GREAT for awhile. I was working out, putting on 30 lbs of muscle, and I had zero issues for about 5 years...until now.
Over the last month or so, I noticed a libido drop. Got tested and the results were bad. You can see the chart I created attached.
Now I'm wondering if my type 2 has become type 1 or mixed. I guess when I re-test LH and FSH, I'll see.
Any thoughts you have would be appreciated. I'm going to push my doctor to get me the right bloodwork and to refer me to a good endo ASAP. Hopefully I don't need to wait 2 months for an appointment.