If taking an AI works for you, then that is a good thing.
There is a strong placebo component in pain and mood clinical studies. That effect wears off in a few weeks. If an AI works for you for more than 2 months, then it works for you.
I think there are several potential factors that may induce irritability in men on TRT:
1- Pre-existing irritability traits. Irritability, in my opinion and experience, comes from feeling we are not in control of our surroundings. It can also be caused by poor sleep, a constant stressor like nagging wife or kids (again, lack of control of your surroundings), financial stress, comparing ourselves to others, and many more factors.
2- TRT shuts down progesterone and most of pregnenolone. These two hormones are tied to calmness, sleep quality and mood. Too bad we do not have data on supplementing either of them or a combination of them.
3- There may be an increase in epinephrine on TRT but I can't find the study now.
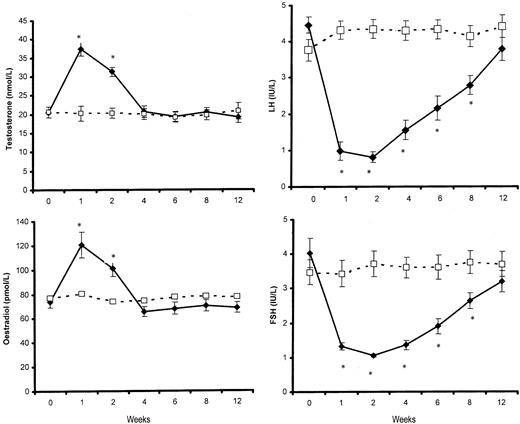
It is unfortunate that we only have a very small study like this one that provided only one injection if Aveed (Nebido). Results would probably be more meaningful with a larger sample size and a year follow up with several injections.
Abstract. The prospects of wider application of testosterone (T) in novel indications such as male contraception have prompted renewed interest in the inve

academic.oup.com
Results of the present study showed that elevation of T to supraphysiological or high normal levels for 2–4 wk had significant minor effects on mood but none on aggressive tendencies or other aspects of behavior such as assertiveness, irritability, self-esteem, or sexual function. Specifically, TU administration was associated with significant increases in the anger-hostility scores from baseline to wk 2, compared with a reduction in anger-hostility over the same time period in the placebo phase. Although this change in anger-hostility is statistically significant, the clinical or pathological significance is uncertain. The mean anger-hostility scores reported at wk 2 (mean = 10.7) are comparable with normative data from college samples in the United States (mean = 10.1) (
33) and with hypogonadal men after T replacement therapy (mean = 10.2) (
27). To further place it in context, impulsive-aggressive individuals who meet the first two diagnostic criteria for intermittent explosive disorder (
45) and have a history of serious assaultive and aggressive acts have been found to score 16.0 on the anger-hostility subscale of the POMS (
46). Therefore, the magnitude of the observed change in the present study is comparatively minor and remained well within the normal range. It is likely to reflect, at most, a subtle response to a transient elevation in circulating T revealed only under closely controlled psychometric monitoring. Nevertheless, future investigations should monitor any potential changes in anger-hostility to rule out clinically significant effects in susceptible individuals, especially after repeated or sustained elevations of T into the supraphysiological range.














 The Ultimate GLP-1 Guide: Weight Loss, Side Effects & Sarcopenia Risk
The Ultimate GLP-1 Guide: Weight Loss, Side Effects & Sarcopenia Risk