Today we’re excited to announce a breakthrough in men’s hormone optimization: Maximus' Oral TRT+ Protocol. Testosterone, without injections or messy creams, all while maintaining fertility markers.

Timestamps:
0:00 - 0:09 - Introduction
0:10 - 3:54 - What is Maximus Oral TRT+?
3:55 - 4:44 - Maximus' Clinical Study Results & Findings
4:45 - 8:09 - Benefits Of Oral TRT+
8:10 - 9:54 - Getting Started On Oral TRT+
9:55 - 10:36 - Is Oral TRT+ Liver & Kidney Safe?
10:37 - 11:41 - How is Oral TRT+ Safe on Fertility Markers?
11:42 - 15:53 - Oral TRT+ Vs Injectable TRT
15:54 - 17:04 - How long does it take Oral TRT+ to start working?
17:05 - 18:18 - Do I need to donate blood on Oral TRT+?
18:19 - 19:37 - Will Oral TRT+ Give me Gynecomastia?
19:38 - Why This Is A Game-changer in mens TRT.
- 00:00 Overview of Maximus Oral TRT+ Protocol
- Introduction to Maximus Oral TRT+ Protocol, a combination of oral native testosterone and enamine.
- Explanation of native testosterone and its distinction from testosterone esters used in traditional TRT.
- Description of enamine as a selective estrogen receptor modulator (SERM) and its benefits in increasing testosterone levels without the side effects of other medications.
- 02:18 Synergy and Benefits of Maximus Oral TRT+ Protocol
- Explanation of the synergy between native testosterone and enamine in mitigating the suppression of LH and FSH levels.
- Benefits of the protocol include significant increases in testosterone levels, improvements in energy, mood, sexual functioning, body composition, and recovery.
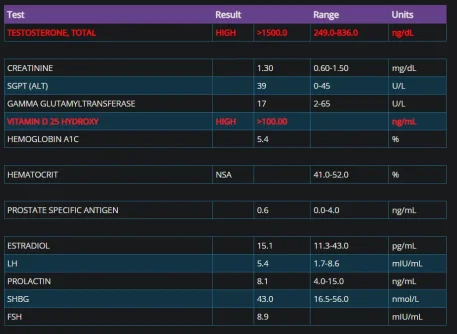
- Clinical trial results showing multiple-fold increases in testosterone levels and improvements in various aspects of well-being for participants.
- 04:55 Side Effects and Management
- 08:21 Process for Getting Started
- Explanation of the process for starting the protocol, including filling out an online assessment, receiving an at-home blood test kit, and consultation with a doctor.
- Overview of ongoing monitoring and support provided by the clinical care team.
- Assurance of safety regarding liver, kidney, and testicular function, with explanations supported by research studies.
- 10:38
 Frequently Asked Questions
Frequently Asked Questions- Addressing common questions about the protocol, including its effects on liver and kidney function, testicular function, and fertility.
- Explanation of why the protocol is considered superior to traditional TRT in terms of convenience, hormonal balance, and long-term health considerations.
- Reassurance regarding the low likelihood of side effects such as polycythemia and gynecomastia with the Maximus Oral TRT+ Protocol.