Good evening,
First post here! Mods, please move to the appropriate section, but I figured this is a good place to post this thread. I will try to be brief (post edit: I lied apparently, sorry for the lengthy rant).
Backstory
- Cannot gain muscle or strength despite being on proper programming, consuming gram of protein/lb of body-weight, religiously tracking calories and very clean eating (and weighing food), trained by friends who were bodybuilders and/or powerlifters, also by trainers not my friends who were powerlifters. I got enough calories, sleep (moderately good, always had sleep issues despite controlling for all factors), stress was minimal. My max weight I capped out at 178lbs, eating 3800 calories and still not gaining weight (or strength). Been at this for six years. Strength always capped out at very pitiful numbers on squat, bench, deadlifts, press.
- Cognition - Lack of focus, clarity, memory problems, sleep issues, always tired, always irritable. A lot of the other symptoms of low testosterone. Got my levels checked in May 2015 when I was at my heaviest (178lbs) results:
Free Testosterone: 349 (Lab range 196 - 636). Note: Free testosterone is estimated from
measured total testosterone and sex hormone-binding globulin using Vermeulen's algorithm.
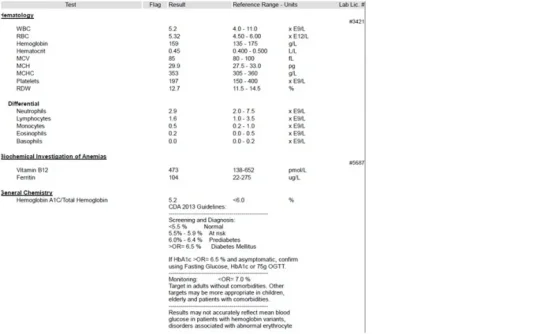
I was told I was normal. Well, I did research a couple of months ago, and nope, not normal. According Vermeulen's research, which while dated, it is still cited everywhere today, I should be at 617ng/dl. So I got my levels tested again. See word doc attached for recent bloodwork. I don't have the older bloodwork in electronic form.
According to online converters, I am at 225ng/dl. Kind of funny, right? Three times less than where I should be. My GP agrees with me about where I should be (I printed off the actual paper, and showed her, and explained this). I have been referred to an endocrinologist for the 28th of January, and suggested I get on testosterone shots.
I am so frustrated (that is an understatement), yet relieved in that I have an answer why I cannot get stronger (or bigger) (along with the cognitive side effects). The endocrinologist will do other bloodwork to determine any compounding factors such as thyroid. I want to know what people here have to say about my recent bloodwork.
Current stats:
Height: 6'0, weight: 160lbs, age: 25, location: Canada eh? body type: small frame and joints, tall and very lanky. Do not have recent bodyfat measurements. When I was 164lbs two months ago, I was according to calipers 11% BF, with 145.757 LBM.
Questions:
- I am a bit scared that these shots will mess up my fertility and have many adverse side effects such as increased risk for liver damage, testicle shrinkage, and prostate cancer.... I do realize that once you go off testosterone, chances of fertility not returning to normal is very low, but it's the other side effects I am worried about. I honestly hope it's a thyroid issue, and I just have to take an oral pill instead of testosterone shots every 10 days). What has been your experiences of side effects?
- Do I have a reasonable case to get my testosterone to 617ng/dl?
Edit: I can't post links or images due to low post count. Any preliminary thoughts are welcome.
First post here! Mods, please move to the appropriate section, but I figured this is a good place to post this thread. I will try to be brief (post edit: I lied apparently, sorry for the lengthy rant).
Backstory
- Cannot gain muscle or strength despite being on proper programming, consuming gram of protein/lb of body-weight, religiously tracking calories and very clean eating (and weighing food), trained by friends who were bodybuilders and/or powerlifters, also by trainers not my friends who were powerlifters. I got enough calories, sleep (moderately good, always had sleep issues despite controlling for all factors), stress was minimal. My max weight I capped out at 178lbs, eating 3800 calories and still not gaining weight (or strength). Been at this for six years. Strength always capped out at very pitiful numbers on squat, bench, deadlifts, press.
- Cognition - Lack of focus, clarity, memory problems, sleep issues, always tired, always irritable. A lot of the other symptoms of low testosterone. Got my levels checked in May 2015 when I was at my heaviest (178lbs) results:
Free Testosterone: 349 (Lab range 196 - 636). Note: Free testosterone is estimated from
measured total testosterone and sex hormone-binding globulin using Vermeulen's algorithm.
I was told I was normal. Well, I did research a couple of months ago, and nope, not normal. According Vermeulen's research, which while dated, it is still cited everywhere today, I should be at 617ng/dl. So I got my levels tested again. See word doc attached for recent bloodwork. I don't have the older bloodwork in electronic form.
According to online converters, I am at 225ng/dl. Kind of funny, right? Three times less than where I should be. My GP agrees with me about where I should be (I printed off the actual paper, and showed her, and explained this). I have been referred to an endocrinologist for the 28th of January, and suggested I get on testosterone shots.
I am so frustrated (that is an understatement), yet relieved in that I have an answer why I cannot get stronger (or bigger) (along with the cognitive side effects). The endocrinologist will do other bloodwork to determine any compounding factors such as thyroid. I want to know what people here have to say about my recent bloodwork.
Current stats:
Height: 6'0, weight: 160lbs, age: 25, location: Canada eh? body type: small frame and joints, tall and very lanky. Do not have recent bodyfat measurements. When I was 164lbs two months ago, I was according to calipers 11% BF, with 145.757 LBM.
Questions:
- I am a bit scared that these shots will mess up my fertility and have many adverse side effects such as increased risk for liver damage, testicle shrinkage, and prostate cancer.... I do realize that once you go off testosterone, chances of fertility not returning to normal is very low, but it's the other side effects I am worried about. I honestly hope it's a thyroid issue, and I just have to take an oral pill instead of testosterone shots every 10 days). What has been your experiences of side effects?
- Do I have a reasonable case to get my testosterone to 617ng/dl?
Edit: I can't post links or images due to low post count. Any preliminary thoughts are welcome.