frankparkway
New Member
My current bloodwork
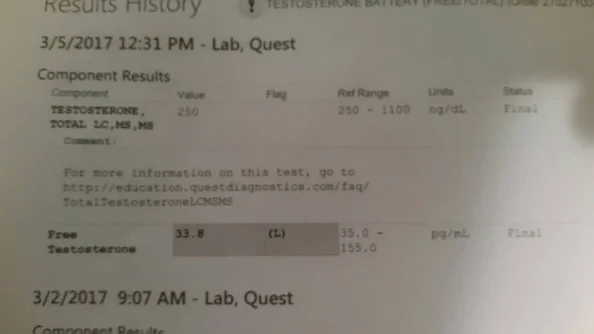
Testosterone, Serum Testosterone, Serum 228 LOW 264-916 ng/dL 01
Luteinizing Hormone(LH), S LH 5.4 NORMAL 1.7-8.6 mIU/mL 01
FSH, Serum FSH 4.9 NORMAL 1.5-12.4 mIU/mL 01
Estradiol Estradiol <5.0 LOW 7.6-42.6 pg/mL 01 Roche ECLIA methodology
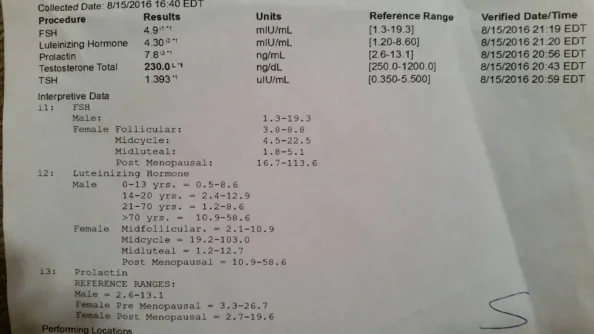
Also I included previous years blood work. 36 years old, fit, muscular, athletic. In the past I have run mild prohormone cycles. Haven't ran any in 2 years. Wondering if I have recovered completely or if I damage my self. Waiting to see a Dr. don't know what specific route I want to go, I don't want to go on TRT if possible.
Testosterone, Serum Testosterone, Serum 228 LOW 264-916 ng/dL 01
Luteinizing Hormone(LH), S LH 5.4 NORMAL 1.7-8.6 mIU/mL 01
FSH, Serum FSH 4.9 NORMAL 1.5-12.4 mIU/mL 01
Estradiol Estradiol <5.0 LOW 7.6-42.6 pg/mL 01 Roche ECLIA methodology
Also I included previous years blood work. 36 years old, fit, muscular, athletic. In the past I have run mild prohormone cycles. Haven't ran any in 2 years. Wondering if I have recovered completely or if I damage my self. Waiting to see a Dr. don't know what specific route I want to go, I don't want to go on TRT if possible.