Your still at this I see.
Need to post more thorough labs.
Always include the reference ranges/assays used TT (LC/MS-MS or direct immunoassay), estradiol (LC/MS-MS or direct immunoassay), FT (Equilibrium Dialysis, Ultrafiltration, direct immunoassay or cFT).
Results can be skewed if you are not using accurate assays especially when it comes to free testosterone.
You left out critical blood markers SHBG, hemoglobin and hematocrit.
What is your protocol 160 mg T once weekly or are you still on twice weekly injections which you were following back in May (thread posted below).
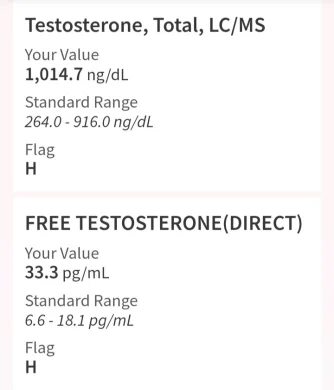
Estradiol: 64.2. (since this result, I started taking arimidex .5 mg (1/2. tablet) twice per week Testosterone total: 1,190 Testosterone free: 25.6 What is the best range for best results? I know the estrogen was too high...

www.excelmale.com
Where your labs done at true trough which would be 7 days post-injection if you are injecting 160 mg T once weekly and if you are injecting 160 mg T split twice weekly (every 3.5 days) than your true trough would be 84 hrs post-injection.
Although TT is important to know FT is what truly matters as it is the active unbound fraction of testosterone responsible for the positive effects.
Even without posting the reference ranges your TT is very high which would have your FT high even if you have highish SHBG.
Top it off that your estradiol is high due to the high FT which is why you threw in the AI.
Keep in mind that if these are your TT, FT and estradiol levels at true trough than peak levels will be much higher.
If such is the case then you would easily have room to lower your weekly dose and drop the AI.
Can be a slippery slope when relying on an aromatase inhibitor to try and manage elevated estradiol as in many cases one can easily crash e2 if they are not careful.
Too many end up overmedicating.
The sensible ones are using micro-doses.
Even then there are many that are running way too high a trough FT level and could easily avoid use of an AI by lowering their dose.
Too many still caught up on that more T is better mentality.
Running too high an FT can be just as bad in the long run as having a low FT in many ways.
As I have stated numerous times on the forum we need to tread lightly when trying to manipulate testosterone metabolites estradiol and DHT as they are needed in healthy amounts and are critical to our overall health.
Estradiol and DHT are needed in healthy amounts to experience the full spectrum of testosterones beneficial effects on mood, energy, libido, erectile function, cardiovascular health, brain, bones, tendons, immune system, body composition, and recovery.
*Natural testosterone is viewed as the best androgen for substitution in hypogonadal men. The reason behind the selection is that testosterone can be converted to DHT and E2, thus developing the full spectrum of testosterone activities in long-term substitution
Looking over your labs back in May your were hitting a very high TT 1190 ng/dL and although your FT was a little lower 25.6 than now 33.3 you never stated what method (assay, calculated) was used or the reference ranges.
Again with a very high TT almost 1200 ng/dL your FT would be high even if you had highish/high SHBG.
You threw in the AI to try and manage your elevated estradiol.
Put money on it that your RBCs, hemoglobin and hematocrit were high back in May and on your current protocol!
My reply from a previous thread may give you some insight when it comes to using/relying on testosterone to treat depression/anxiety.
*Although TRT can improve mild depression, anxiety, and overall well-being it is highly doubtful that it will have a big impact on treating MDD.
*Keep in mind that even men with healthy testosterone levels can still suffer from mild, moderate, or severe depression.
Hi! I been struggling with ptsd and depression for a few years as a result of years of working as a first responder. I sought different ways to fix it however they work temporarily. Two weeks ago I got some blood work done and my testosterone came back low the doctor referred me to a...
www.excelmale.com