Ok jumping back on because it’s been a while. Been running 100mg spread over two doses every 3.5 days (60/40 mg) since I last posted. Been feeling ok, steady. Wondering if dose could go up. Couple things here. Got labs back yesterday (all except E2, Sensitive test takes longer) . I’ve got a two part
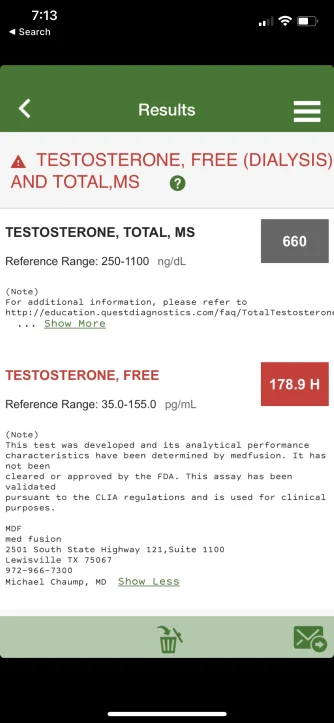
total test - 660
Free test - 179
SHBG - 15
thoughts on increasing to 120mg week?
2nd question - after 4 month waiting period I did go see Dr. Larry
Lipshultz in Houston and he’s recommending I start on 200mg week injected once weekly with a 1mg dose of anastrozole per week. I have to admit I was shocked to hear him say this, that doesn’t seem like the right step considering he is supposed to be a leader in the field. Any thoughts on him / his recommendation?












 Daily Injections Causing Huge RBC Spike? Why?
Daily Injections Causing Huge RBC Spike? Why?