madman
Super Moderator
Learning objectives
Background
Erectile dysfunction (ED) is defined as the inability to attain or maintain a penile erection of sufficient quality to allow satisfactory sexual performance.
The prevalence of this condition increases with age with a 39% prevalence at the age of 40 years and a 67% prevalence at the age of 70 years. It has been estimated that the worldwide prevalence of erectile dysfunction will be 322 million cases by the year 2025.
Fig. 1: Physiology of Penile Erection. NO: Nitric Oxide. GTP:guanosine triphosphate PDE5 phosphodiesterase type 5. cGMP: cyclic guanosine monophosphate.
References: Radiology, Hospital Fundación Jiménez Díaz, Hospital Universitario Fundación Jiménez díaz - Madrid/ES
.png")
Fig. 2: Veno-occlusive mechanism in penile erection. A- Normal flacid penis. Smooth muscle cells are contracted and the sinusoid spaces in corpus cavernosum are empty. B- Normal erect penile anatomy. The increase of NO levels allows smooth muscle cells relaxation, sinusoid spaces are enlarged and compress the subtunical venous plexus. C-Several mechanism of venogenic erectile dysfunction.
References: McVary KT. Erectile Dysfunction. N Engl J Med 2007;357:2472-81.
Fig. 3: Main Causes of Erectile Dysfunction.
Fig. 4: Risk Factors in Erectile Dysfunction. Endothelial Dysfunction as a shared physiopathological mechanism between ED and cardiovascular diseases.
References: Radiology, Hospital Fundación Jiménez Díaz, Hospital Universitario Fundación Jiménez díaz - Madrid/ES
Fig. 5: The Hypothesis of Arterial Diameter. - Given coronary arteries diameter, myocardial vascularisation would be affected secondarily after penile vascularisation. - Coronary Arteries Diseases and Erectile Dysfunction:different clinical signs of same progressive disease.
References: Montorsi P et al. (2003). Eur Urol ; 44: 352-354.
- Learn about erectile dysfunction. Pathophysiology, symptoms and main causes.
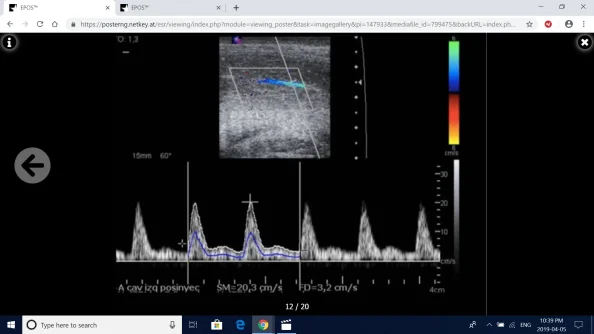
- Stimulated Color Doppler ultrasound diagnostic criteria. Arteriogenic erectile dysfunction, veno-occlusive erectile dysfunction , mixed aetiology and false venous-leak.
- Role of interventional radiology in the treatment of venous-leak.
- Endovascular embolisation therapy.
Background
Erectile dysfunction (ED) is defined as the inability to attain or maintain a penile erection of sufficient quality to allow satisfactory sexual performance.
The prevalence of this condition increases with age with a 39% prevalence at the age of 40 years and a 67% prevalence at the age of 70 years. It has been estimated that the worldwide prevalence of erectile dysfunction will be 322 million cases by the year 2025.
Fig. 1: Physiology of Penile Erection. NO: Nitric Oxide. GTP:guanosine triphosphate PDE5 phosphodiesterase type 5. cGMP: cyclic guanosine monophosphate.
References: Radiology, Hospital Fundación Jiménez Díaz, Hospital Universitario Fundación Jiménez díaz - Madrid/ES
Fig. 2: Veno-occlusive mechanism in penile erection. A- Normal flacid penis. Smooth muscle cells are contracted and the sinusoid spaces in corpus cavernosum are empty. B- Normal erect penile anatomy. The increase of NO levels allows smooth muscle cells relaxation, sinusoid spaces are enlarged and compress the subtunical venous plexus. C-Several mechanism of venogenic erectile dysfunction.
References: McVary KT. Erectile Dysfunction. N Engl J Med 2007;357:2472-81.
Fig. 3: Main Causes of Erectile Dysfunction.
Fig. 4: Risk Factors in Erectile Dysfunction. Endothelial Dysfunction as a shared physiopathological mechanism between ED and cardiovascular diseases.
References: Radiology, Hospital Fundación Jiménez Díaz, Hospital Universitario Fundación Jiménez díaz - Madrid/ES
Fig. 5: The Hypothesis of Arterial Diameter. - Given coronary arteries diameter, myocardial vascularisation would be affected secondarily after penile vascularisation. - Coronary Arteries Diseases and Erectile Dysfunction:different clinical signs of same progressive disease.
References: Montorsi P et al. (2003). Eur Urol ; 44: 352-354.