

Nelson Vergel
Founder, ExcelMale.com
Human Chorionic Gonadotropin, Pregnenolone and DHEA – By Gene Devine
Below is a paper I’ve written after much research and study on why men need HCG, Pregnenolone and DHEA while on a Testosterone Replacement Protocol. I have known men who have printed this out and given to their Physician who would not prescribe HCG but after reading this agreed to prescribing it. It’s an easy read and very informative and if you are not on HCG as part of your TRT protocol this may go to help you understand why it is important for your overall health and well-being.
When a man introduces Testosterone exogenously it significantly changes how the Hypothalamus(H), Pituitary(P) and Testicle(T) glands react to each other in keeping men’s androgenic hormones in balance. Many of our hormones act in a cascading event and the axis between the these three glands are no different.

When T levels are low in a normal healthy man the Hypothalamus releases a “releasing” hormone (LHRH) that tells the Pituitary to release another hormone known as Luteinizing Hormone (LH). In turn, LH reaches the receptors on the Leydig cells within the testicles telling them to do their thing among which is the production of Pregnenelone from Cholesterol, Sperm and Testosterone among other things needed downstream in all hormonal pathways.
Exogenous Testosterone halts the HPT Axis (HPTA) and as such the testicles are no longer receiving LH. This is know by most of us as simply “shutdown” or “HPTA suppression.”
In order for men on a TRT protocol where they are in a state of shutdown/suppression to make up for the lost production of LH they will need add hCG to their protocol which is a bioidentical form of LH (LH Analog).
hCG (http://en.wikipedia.org/wiki/Human_c…c_gonadotropin) is a water based peptide hormone that can only be injected to replace the lost LH hormone that a TRT protocol shuts down. There are “so called” oral forms of hCG that some men are placed on, or purchased from other sources, but from all that I read it’s not possible to injest hCG and get it past the liver to make its efficacy plausible. Recently, oral micronized verions of hCG are available by prescription and have shown to be a successful alternative to injections for some men…talk to your Doctor.
So what happens when a man testicles don’t function anymore do to the lack of LH?
The Biggie: Testicular Atrophy. Men will see their testes get smaller over time and hurt constantly along the way. The duration for this event seems to be different in men where younger guys can seem to go longer where mid to older guys see the event happens on a more accelerated scale. Some think it happens to do with the amount of receptors on the Leydig cells…but who really knows.
Sperm production is pretty much halted.
Men’s scrotum’s will get really tight and pull up against the body causing pain and end up looking like a 5 year old.
The testes are the single largest producer of the hormone Pregnenelone; the mother of all hormones (http://www.antiaging-systems.com/165…one-metabolite) We need Pregnenelone for so many reasons (read the link here) and while it can be supplemented it’s hit or miss on how effective supplementation can be for some men.
Why we need hCG:
1. IMPORTANT: To produce Pregnenelone; hCG activates the p450 side chain cleavage (p450scc) enzyme which converts cholesterol to Pregnenelone!!! (Read the link above, please.)
2. To produce the precursors for DHEA, Estrogen, Cortisol, Testosterone and DHT…back filling the pathways (See #1 above)
3. For proper and normal brain function
4. For proper functioning of the testicles
5. If men ever want to restart
6. If men ever want to have children
7. If men don’t want balls that end up in a small mass of useless Collagen
8. The list goes on…
In short, hCG keeps the testicles functioning in a normal state and supports all three metabolic pathways. It prevents Pregnenelone deficiency and supporting all our other CHOL pathways and hormones as well.
As we’ve all seen first hand in this community; when a man on a TRT protocol is not on hCG they complain of shrinking testicle and the accompanying pain that goes with it.
But when they start on hCG (because of all the things listed above and more) they all state how much better they feel and the pain associated with their testicular atrophy subsiding and that their testicles feel much better as well.
Does a man need hCG on a TRT protocol?
Nope.
But for all the reasons above a man should be made aware of why hCG and Human chorionic gonadotropin are important to their health and well being on a life long journey of TRT.
The efficacy for hCG for both Primary and Secondary Hypogonadism has been documented. For those whose Doctor refuses to prescribe HCG as part of your TRT protocol print this study abstract and force them to read it:
Tung-Chin Hsieh, Alexander W. Pastuszak, Kathleen Hwang and Larry I. Lipshultz*,†
From the Division of Urology, University of California-San Diego (TCH), San Diego, California, Scott Department of Urology, Baylor College of Medicine (AWP, LIL), Houston, Texas, and Department of Urology (KH), Brown University School of Medicine, Providence, Rhode Island
Purpose: Testosterone replacement therapy results in decreased serum gonadotropins and intratesticular testosterone , and impairs spermatogenesis, leading to azoospermia in 40% of patients. However, intratesticular testosterone can be maintained during testosterone replacement therapy with co-administration of low dose human chorionic gonadotropin , which may support continued spermatogenesis in patients on testosterone replacement therapy.
Materials and Methods: We retrospectively reviewed the records of hypogonadal men treated with testosterone replacement therapy and concomitant low dose human chorionic gonadotropin (HCG ). Testosterone replacement consisted of daily topical gel or weekly intramuscular injection with intramuscular human chorionic gonadotro- pin (500 IU) every other day. Serum and free testosterone, estradiol, semen parameters and pregnancy rates were evaluated before and during therapy.
Results: A total of 26 men with a mean age of 35.9 years were included in the study. Mean followup was 6.2 months. Of the men 19 were treated with injectable testosterone and 7 were treated with transdermal gel. Mean serum hormone levels before vs during treatment were testosterone 207.2 vs 1,055.5 ng/dl (p <0.0001), free testosterone 8.1 vs 20.4 pg/ml (p = 0.02) and estradiol 2.2 vs 3.7 pg/ml (p = 0.11). Pretreatment semen parameters were volume 2.9 ml, density 35.2 million per ml, motility 49.0% and forward progression 2.3. No differences in semen parameters were observed during greater than 1 year of followup. No impact on semen parameters was observed as a function of testosterone formulation. No patient became azoospermic during concomitant testosterone replacement and human chorionic gonadotropin therapy. Nine of 26 men contributed to pregnancy with the partner during follow-up.
Conclusions: Low dose human chorionic gonadotropin appears to maintain semen parameters in hypogonadal men on testosterone replacement therapy. Concurrent testosterone replacement and human chorionic gonadotropin use may preserve fertility in hypogonadal males who desire fertility preservation while on testosterone replacement therapy.
hCG Injection Protocols
Let’s start by saying that there are no hard and fast rules for hCG injection protocols. There are a number of well known Physicians who have recommendations and prescribe based on their experience with patient’s subjective responses to treatment and subsequent serum levels. There are other variables as well that need to be taking into consideration when contemplating hCG injection protocols like whether or not the man is Primary or Secondary Hypogonadal can determine hCG injection protocols.
That being said, there are a number of hCG injection protocols that appear more commonly and are based on Testosterone injection frequency and or the use of a cream or gel.
Note: It’s not advisable to inject more then 500iu’s of hCG in any 24 hour period as it can increase intratesticular E2 which an AI is largely ineffective in controlling. Additionally, there is a theory that large amounts of hCG may desensitize the receptors on the lydeg cells.
Once a Week Testosterone Injection Protocols
If a man injects Testosterone on a once a week basis the more common protocol is to use 250IU of hCG two days before and one day before their next testosterone injection. The theory here is that Testosterone serum levels are at near half life and the injection of hCG on these days increase natural production creating a bridge until the next testosterone injection.
Twice a Week Testosterone Injections
If a man injects twice a week similar to an every 3.5 day schedule the more common protocol are smaller doses more frequently. It’s not uncommon to see men inject 250IU of hCG on an EOD basis or on a Monday-Wednesday-Friday protocol.
Cream or Gel Daily Use
If a man uses a Cream and/or Gel some of the top Testosterone Replacement Physicians, like Dr. John Crisler, recommend patients use 100iu of hCG every day.
hCG Injections
Injecting hCG prevents a drug induced Human chorionic gonadotropin deficiency and helps support the other androgen pathways as well. When men are on a TRT protocol without hCG and then add in hCG many report a significant improvement in mood that many attribute to restored Human chorionic gonadotropin levels.
When injecting hCG, you inject into the fat under the skin just the same as diabetics inject insulin. The product literature is all about use a fertility drug for women with large IM [injected into muscle] doses. There is no need for men to inject hCG IM.
Research using SC injections in men has demonstrated the effectiveness of the 350 iu EOD dosing. You can seek diabetic patient educational material for insulin injection techniques to use for hCG and/or testosterone injections.
Pregnenolone – Why You Need It
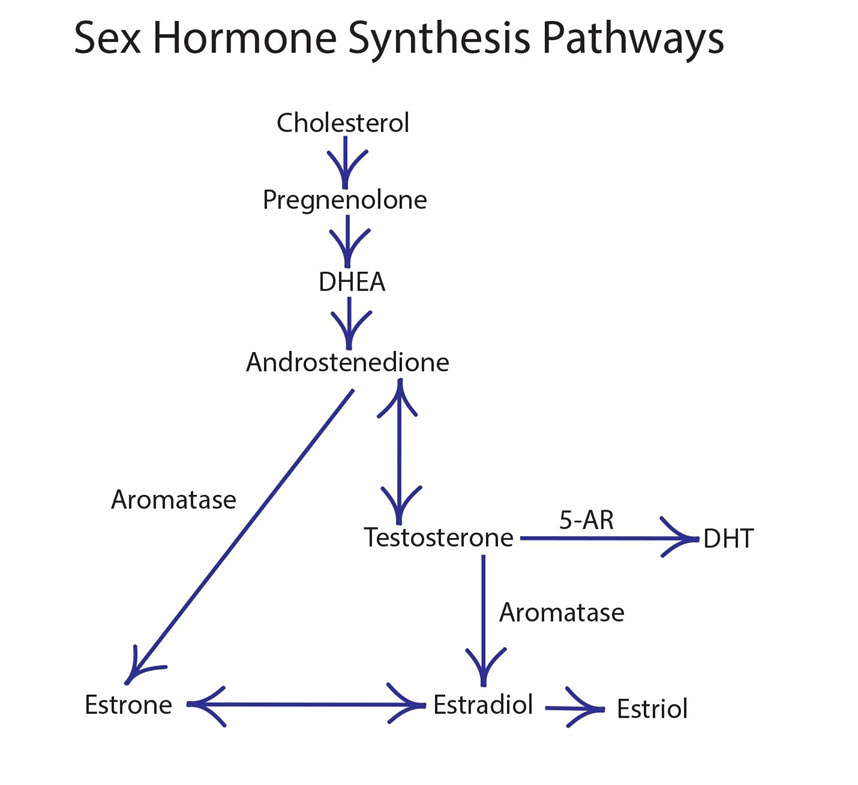
Pregnenolone is a hormone that many Doctors and men are not familiar with or understand it’s role in the CHOL pathways but it’s critically important to our health as it is a “precursor hormone” to all other hormones. Restoring Pregnenolone to optimal levels is important but seems to get the least attention by Doctors. Remember, the testes are the single largest producer of the hormone Pregnenolone. Pregnenolone is important for proper mental functioning and is the precursor to all of the steroid hormones found in the three CHOL pathways such as DHEA, testosterone, DHT, estrogen, cortisol…
So what are the benefits of Pregnenolone?
In our bodies Pregnenelone is manufactured by cholesterol (CHOL). The hormone performs many functions in a man’s body, including:
Promotes healthy brain function and protects against dementia and Alzheimer’s disease. Many men state feeling good when they start supplementing Human chorionic gonadotropin.
It can also prevent age related diseases and support the Central Nervous System (CNS).
Boosts the immune system and increases energy produciton.
Protects against coronary disease and improves heart health and can lower cholesterol levels.
Enhances mood and relieves depression. Many men state their mood betters when they start supplementation.
Relieves arthritis pain!
Fights the effects of fatigue and stress.
The optimal serum levels for Pregnenelone is 180 ng/dl for men. Pregnenolone can be purchased over the counter in a pill (micronized slow release is the best for pills) or sublingual form in addition to transdermal creams. A typical dose is 50 to 200 mg daily best taken in the morning on an empty stomach (cream applied in the morning as well). Pregnenolone is considered safe and because is converts to DHEA which leads to other hormones it’s best to get your Pregnenolone levels tested before supplementing.
DHEA Supplementation
Dehydroepiandrosterone: DHEA
As presented by Dr. Neal Rouzier, M.D.
Here’s a great reason to add DHEA to your protocol.
DHEA is a hormone secreted primarily by the adrenal glands. It results in a shift of a catabolic state to an anabolic or protein building state.
It reduces cardiovascular risks by increasing lipolyses (decrease visceral fat).
It stimulates the immune system, restores sexual vitality, improves moods, decreases cholesterol and body fat.
It improves memory, increases energy, and has anti-cancer properties by enhancing the immune system.
It is an endocrine precursor to other hormones, prevents immuno-senescence, loss of sleep, osteoporosis, atherosclerosis.
DHEA reduces insulin requirement
Adrenal hormone anabolic vs. catabolic metabolism
Restores immunity
Prevents osteoporosis, increases bone density
Prevents cancer in lab animals
Prevents diabetes & heart disease
Decreases visceral fat
Improves mood & well-being
Improves energy & memory
Slows aging process in lab animals
Prevents lipid peroxidation = antioxidant
Endocrine precursor to T.P.E.
7-keto DHEA is not a precursor to other HRT = avoid
Neurotransmitter (recently discovered)
Presently pending FDA approval for Lupus (Prasterone)
Clinically substantiated uses of DHEA include replacement for:
Low DHEA levels
Chronic disease
Adrenal exhaustion or corticosteroid therapy
SLE
Improving bone density
Improving depression & mood disorders
Enhancing immune response by activating T-cells
Improving well-being
Decreasing cardiovascular risk
Improving erectile dysfunction
Anyone over 40
DHEA has never been shown to reverse the aging process
Nevertheless DHEA is important for preventive medicine
DHEA inhibits synthesis of thromboxane A2, reduces plasminogen activator inhibitor, and tissue plasminogen activator
– all decreasing platelet aggregation and ischemia.
Administration:
Men<200lb: 50mg AM
Men>200lb: 75-100mg AM
Women <50yo: 10-15mg AM
Women >50yo: 25mg AM
IMPORTANT:
DHEA Serum Levels
MEN
Range 100-600
Optimal 500-600
WOMEN
Range 50-300
Optimal 200-250
Higher levels in women predispose them to side effects – therefore stay low
Monitor monthly until optimal
Assure correct dose and compliance
Measure DHEA-S and not DHEA
Side effects: acne, hirsutism
Tx: Lower dose or take QOD Spironolactone 100 mg/day
Contraindicated in sex hormone responsive tumors – breast, ovarian, uterine, prostate
Conversion to T.P.E.?
DHEA raises testosterone levels in women slightly, yet not in men
DHEA raises estradiol slightly in men
Indications:
Over age 40 for health protection
Preventive medicine and well-being
Symptoms of aging, mood & depression
‘Cause the medical literature suggests it if we want to live longer, happier, healthier
DHEA – S04 MEN Blood levels
Optimal : 500-600 ug/ml
Side effects rare in men
WOMEN
Optimal : 200-250 ug/ml
Dose based on side effects
Side effects very common in women
DHEA Dose MEN
Capsule – SR micronized
50 mg Q am
>200 lbs – 75 – 100 mg Q am
WOMEN Capsule – SR micronized
10 mg Q am if over 40
15 mg Q am if over 50
25 mg Q am if over 60
If under age 40, do not prescribe due to sensitivity causing side effects.
The post Human Chorionic Gonadotropin, Pregnenolone and DHEA appeared first on Testosterone Wisdom.
Continue reading...
Below is a paper I’ve written after much research and study on why men need HCG, Pregnenolone and DHEA while on a Testosterone Replacement Protocol. I have known men who have printed this out and given to their Physician who would not prescribe HCG but after reading this agreed to prescribing it. It’s an easy read and very informative and if you are not on HCG as part of your TRT protocol this may go to help you understand why it is important for your overall health and well-being.
When a man introduces Testosterone exogenously it significantly changes how the Hypothalamus(H), Pituitary(P) and Testicle(T) glands react to each other in keeping men’s androgenic hormones in balance. Many of our hormones act in a cascading event and the axis between the these three glands are no different.
When T levels are low in a normal healthy man the Hypothalamus releases a “releasing” hormone (LHRH) that tells the Pituitary to release another hormone known as Luteinizing Hormone (LH). In turn, LH reaches the receptors on the Leydig cells within the testicles telling them to do their thing among which is the production of Pregnenelone from Cholesterol, Sperm and Testosterone among other things needed downstream in all hormonal pathways.
Exogenous Testosterone halts the HPT Axis (HPTA) and as such the testicles are no longer receiving LH. This is know by most of us as simply “shutdown” or “HPTA suppression.”
In order for men on a TRT protocol where they are in a state of shutdown/suppression to make up for the lost production of LH they will need add hCG to their protocol which is a bioidentical form of LH (LH Analog).
hCG (http://en.wikipedia.org/wiki/Human_c…c_gonadotropin) is a water based peptide hormone that can only be injected to replace the lost LH hormone that a TRT protocol shuts down. There are “so called” oral forms of hCG that some men are placed on, or purchased from other sources, but from all that I read it’s not possible to injest hCG and get it past the liver to make its efficacy plausible. Recently, oral micronized verions of hCG are available by prescription and have shown to be a successful alternative to injections for some men…talk to your Doctor.
So what happens when a man testicles don’t function anymore do to the lack of LH?
The Biggie: Testicular Atrophy. Men will see their testes get smaller over time and hurt constantly along the way. The duration for this event seems to be different in men where younger guys can seem to go longer where mid to older guys see the event happens on a more accelerated scale. Some think it happens to do with the amount of receptors on the Leydig cells…but who really knows.
Sperm production is pretty much halted.
Men’s scrotum’s will get really tight and pull up against the body causing pain and end up looking like a 5 year old.
The testes are the single largest producer of the hormone Pregnenelone; the mother of all hormones (http://www.antiaging-systems.com/165…one-metabolite) We need Pregnenelone for so many reasons (read the link here) and while it can be supplemented it’s hit or miss on how effective supplementation can be for some men.
Why we need hCG:
1. IMPORTANT: To produce Pregnenelone; hCG activates the p450 side chain cleavage (p450scc) enzyme which converts cholesterol to Pregnenelone!!! (Read the link above, please.)
2. To produce the precursors for DHEA, Estrogen, Cortisol, Testosterone and DHT…back filling the pathways (See #1 above)
3. For proper and normal brain function
4. For proper functioning of the testicles
5. If men ever want to restart
6. If men ever want to have children
7. If men don’t want balls that end up in a small mass of useless Collagen
8. The list goes on…
In short, hCG keeps the testicles functioning in a normal state and supports all three metabolic pathways. It prevents Pregnenelone deficiency and supporting all our other CHOL pathways and hormones as well.
As we’ve all seen first hand in this community; when a man on a TRT protocol is not on hCG they complain of shrinking testicle and the accompanying pain that goes with it.
But when they start on hCG (because of all the things listed above and more) they all state how much better they feel and the pain associated with their testicular atrophy subsiding and that their testicles feel much better as well.
Does a man need hCG on a TRT protocol?
Nope.
But for all the reasons above a man should be made aware of why hCG and Human chorionic gonadotropin are important to their health and well being on a life long journey of TRT.
The efficacy for hCG for both Primary and Secondary Hypogonadism has been documented. For those whose Doctor refuses to prescribe HCG as part of your TRT protocol print this study abstract and force them to read it:
Concomitant Intramuscular Human Chorionic Gonadotropin Preserves Spermatogenesis in Men Undergoing Testosterone Replacement Therapy
Tung-Chin Hsieh, Alexander W. Pastuszak, Kathleen Hwang and Larry I. Lipshultz*,†
From the Division of Urology, University of California-San Diego (TCH), San Diego, California, Scott Department of Urology, Baylor College of Medicine (AWP, LIL), Houston, Texas, and Department of Urology (KH), Brown University School of Medicine, Providence, Rhode Island
Purpose: Testosterone replacement therapy results in decreased serum gonadotropins and intratesticular testosterone , and impairs spermatogenesis, leading to azoospermia in 40% of patients. However, intratesticular testosterone can be maintained during testosterone replacement therapy with co-administration of low dose human chorionic gonadotropin , which may support continued spermatogenesis in patients on testosterone replacement therapy.
Materials and Methods: We retrospectively reviewed the records of hypogonadal men treated with testosterone replacement therapy and concomitant low dose human chorionic gonadotropin (HCG ). Testosterone replacement consisted of daily topical gel or weekly intramuscular injection with intramuscular human chorionic gonadotro- pin (500 IU) every other day. Serum and free testosterone, estradiol, semen parameters and pregnancy rates were evaluated before and during therapy.
Results: A total of 26 men with a mean age of 35.9 years were included in the study. Mean followup was 6.2 months. Of the men 19 were treated with injectable testosterone and 7 were treated with transdermal gel. Mean serum hormone levels before vs during treatment were testosterone 207.2 vs 1,055.5 ng/dl (p <0.0001), free testosterone 8.1 vs 20.4 pg/ml (p = 0.02) and estradiol 2.2 vs 3.7 pg/ml (p = 0.11). Pretreatment semen parameters were volume 2.9 ml, density 35.2 million per ml, motility 49.0% and forward progression 2.3. No differences in semen parameters were observed during greater than 1 year of followup. No impact on semen parameters was observed as a function of testosterone formulation. No patient became azoospermic during concomitant testosterone replacement and human chorionic gonadotropin therapy. Nine of 26 men contributed to pregnancy with the partner during follow-up.
Conclusions: Low dose human chorionic gonadotropin appears to maintain semen parameters in hypogonadal men on testosterone replacement therapy. Concurrent testosterone replacement and human chorionic gonadotropin use may preserve fertility in hypogonadal males who desire fertility preservation while on testosterone replacement therapy.
hCG Injection Protocols
Let’s start by saying that there are no hard and fast rules for hCG injection protocols. There are a number of well known Physicians who have recommendations and prescribe based on their experience with patient’s subjective responses to treatment and subsequent serum levels. There are other variables as well that need to be taking into consideration when contemplating hCG injection protocols like whether or not the man is Primary or Secondary Hypogonadal can determine hCG injection protocols.
That being said, there are a number of hCG injection protocols that appear more commonly and are based on Testosterone injection frequency and or the use of a cream or gel.
Note: It’s not advisable to inject more then 500iu’s of hCG in any 24 hour period as it can increase intratesticular E2 which an AI is largely ineffective in controlling. Additionally, there is a theory that large amounts of hCG may desensitize the receptors on the lydeg cells.
Once a Week Testosterone Injection Protocols
If a man injects Testosterone on a once a week basis the more common protocol is to use 250IU of hCG two days before and one day before their next testosterone injection. The theory here is that Testosterone serum levels are at near half life and the injection of hCG on these days increase natural production creating a bridge until the next testosterone injection.
Twice a Week Testosterone Injections
If a man injects twice a week similar to an every 3.5 day schedule the more common protocol are smaller doses more frequently. It’s not uncommon to see men inject 250IU of hCG on an EOD basis or on a Monday-Wednesday-Friday protocol.
Cream or Gel Daily Use
If a man uses a Cream and/or Gel some of the top Testosterone Replacement Physicians, like Dr. John Crisler, recommend patients use 100iu of hCG every day.
hCG Injections
Injecting hCG prevents a drug induced Human chorionic gonadotropin deficiency and helps support the other androgen pathways as well. When men are on a TRT protocol without hCG and then add in hCG many report a significant improvement in mood that many attribute to restored Human chorionic gonadotropin levels.
When injecting hCG, you inject into the fat under the skin just the same as diabetics inject insulin. The product literature is all about use a fertility drug for women with large IM [injected into muscle] doses. There is no need for men to inject hCG IM.
Research using SC injections in men has demonstrated the effectiveness of the 350 iu EOD dosing. You can seek diabetic patient educational material for insulin injection techniques to use for hCG and/or testosterone injections.
Pregnenolone – Why You Need It
Pregnenolone is a hormone that many Doctors and men are not familiar with or understand it’s role in the CHOL pathways but it’s critically important to our health as it is a “precursor hormone” to all other hormones. Restoring Pregnenolone to optimal levels is important but seems to get the least attention by Doctors. Remember, the testes are the single largest producer of the hormone Pregnenolone. Pregnenolone is important for proper mental functioning and is the precursor to all of the steroid hormones found in the three CHOL pathways such as DHEA, testosterone, DHT, estrogen, cortisol…
So what are the benefits of Pregnenolone?
In our bodies Pregnenelone is manufactured by cholesterol (CHOL). The hormone performs many functions in a man’s body, including:
Promotes healthy brain function and protects against dementia and Alzheimer’s disease. Many men state feeling good when they start supplementing Human chorionic gonadotropin.
It can also prevent age related diseases and support the Central Nervous System (CNS).
Boosts the immune system and increases energy produciton.
Protects against coronary disease and improves heart health and can lower cholesterol levels.
Enhances mood and relieves depression. Many men state their mood betters when they start supplementation.
Relieves arthritis pain!
Fights the effects of fatigue and stress.
The optimal serum levels for Pregnenelone is 180 ng/dl for men. Pregnenolone can be purchased over the counter in a pill (micronized slow release is the best for pills) or sublingual form in addition to transdermal creams. A typical dose is 50 to 200 mg daily best taken in the morning on an empty stomach (cream applied in the morning as well). Pregnenolone is considered safe and because is converts to DHEA which leads to other hormones it’s best to get your Pregnenolone levels tested before supplementing.
DHEA Supplementation
Dehydroepiandrosterone: DHEA
As presented by Dr. Neal Rouzier, M.D.
Here’s a great reason to add DHEA to your protocol.
DHEA is a hormone secreted primarily by the adrenal glands. It results in a shift of a catabolic state to an anabolic or protein building state.
It reduces cardiovascular risks by increasing lipolyses (decrease visceral fat).
It stimulates the immune system, restores sexual vitality, improves moods, decreases cholesterol and body fat.
It improves memory, increases energy, and has anti-cancer properties by enhancing the immune system.
It is an endocrine precursor to other hormones, prevents immuno-senescence, loss of sleep, osteoporosis, atherosclerosis.
DHEA reduces insulin requirement
Adrenal hormone anabolic vs. catabolic metabolism
Restores immunity
Prevents osteoporosis, increases bone density
Prevents cancer in lab animals
Prevents diabetes & heart disease
Decreases visceral fat
Improves mood & well-being
Improves energy & memory
Slows aging process in lab animals
Prevents lipid peroxidation = antioxidant
Endocrine precursor to T.P.E.
7-keto DHEA is not a precursor to other HRT = avoid
Neurotransmitter (recently discovered)
Presently pending FDA approval for Lupus (Prasterone)
Clinically substantiated uses of DHEA include replacement for:
Low DHEA levels
Chronic disease
Adrenal exhaustion or corticosteroid therapy
SLE
Improving bone density
Improving depression & mood disorders
Enhancing immune response by activating T-cells
Improving well-being
Decreasing cardiovascular risk
Improving erectile dysfunction
Anyone over 40
DHEA has never been shown to reverse the aging process
Nevertheless DHEA is important for preventive medicine
DHEA inhibits synthesis of thromboxane A2, reduces plasminogen activator inhibitor, and tissue plasminogen activator
– all decreasing platelet aggregation and ischemia.
Administration:
Men<200lb: 50mg AM
Men>200lb: 75-100mg AM
Women <50yo: 10-15mg AM
Women >50yo: 25mg AM
IMPORTANT:
DHEA Serum Levels
MEN
Range 100-600
Optimal 500-600
WOMEN
Range 50-300
Optimal 200-250
Higher levels in women predispose them to side effects – therefore stay low
Monitor monthly until optimal
Assure correct dose and compliance
Measure DHEA-S and not DHEA
Side effects: acne, hirsutism
Tx: Lower dose or take QOD Spironolactone 100 mg/day
Contraindicated in sex hormone responsive tumors – breast, ovarian, uterine, prostate
Conversion to T.P.E.?
DHEA raises testosterone levels in women slightly, yet not in men
DHEA raises estradiol slightly in men
Indications:
Over age 40 for health protection
Preventive medicine and well-being
Symptoms of aging, mood & depression
‘Cause the medical literature suggests it if we want to live longer, happier, healthier
DHEA – S04 MEN Blood levels
Optimal : 500-600 ug/ml
Side effects rare in men
WOMEN
Optimal : 200-250 ug/ml
Dose based on side effects
Side effects very common in women
DHEA Dose MEN
Capsule – SR micronized
50 mg Q am
>200 lbs – 75 – 100 mg Q am
WOMEN Capsule – SR micronized
10 mg Q am if over 40
15 mg Q am if over 50
25 mg Q am if over 60
If under age 40, do not prescribe due to sensitivity causing side effects.
The post Human Chorionic Gonadotropin, Pregnenolone and DHEA appeared first on Testosterone Wisdom.
Continue reading...











