During adolescence, androgens are responsible for the development of secondary sexual characteristics, pubertal growth, and the anabolic effects on bone and muscle mass.Testosterone is the most abundant testicular androgen, but some effects are mediated by its conversion to the more potent androgen dihydrotestosterone (DHT) or to estradiol. Androgen deficiency, requiring replacement therapy, may occur due to a primary testicular failure or secondary to a hypothalamic–pituitary disorder. A very frequent condition characterized by a late activation of the gonadal axis that may also need androgen treatment is constitutional delay of puberty.Of the several testosterone or DHT formulations commercially available, very few are employed, and none is marketed for its use in adolescents.The most frequently used androgen therapy is based on the intramuscular administration of testosterone enanthate or cypionate every 3 to 4 weeks, with initially low doses. These are progressively increased during several months or years, in order to mimic the physiology of puberty, until adult doses are attained. Scarce experience exists with oral or transdermal formulations. Preparations containing DHT, which are not widely available, are preferred in specific conditions. Oxandrolone, a non-aromatizable drug with higher anabolic than androgenic effects, has been used in adolescents with preserved testosterone production, like Klinefelter syndrome, with positive effects on cardiometabolic health and visual, motor, and psychosocial functions. The usual protocols applied for androgen therapy in boys and adolescents are discussed.
Figure 3. Schematic of serum testosterone levels in hypogonadal adult males before (time 0) and after having received intramuscular injections of testosterone undecanoate (1,000 mg) or enanthate (250 mg). The graded area represents normal serum levels of testosterone for an adult male. Unfortunately, no data are available for boys or adolescents. Data obtained from Di Luigi et al. (2009), Morgentaler et al. (2008), Nieschlag and Behre (2010), and Zhang et al. (1998).
Wow!! one time use of testosterone in early fetal and late fetal stages!! How do they know the boy has a micropenis before being born? Is ultrasound that accurate?
Wow!! one time use of testosterone in early fetal and late fetal stages!! How do they know the boy has a micropenis before being born? Is ultrasound that accurate?
Newborns and untreated infants and children with signs of congenital hypoandrogenism due to primary hypogonadism leading to DSD or to primary or central hypogonadism leading to micropenis and cryptorchidism in the context of male genitalia may require transient androgen therapy (Hatipoğlu & Kurtoğlu, 2013; Ladjouze & Donaldson, 2019; A. D. Rogol, 2005a,b; Wisniewski et al., 2019). The main aims are penile enlargement and the enhancement of scrotal trophism.
The most usual practice is to give three IM doses of testosterone enanthate 25 mg every 3–4 weeks (Hatipoğlu & Kurtoğlu, 2013; Ladjouze & Donaldson, 2019; A. D. Rogol, 2005a,b; Wisniewski et al., 2019). It should be stressed that this may prove difficult, given that these oil preparations contain 200 or 250 mg in 1–2 ml. Side effects are pain and infections in the injection site, erections, and acne. These low doses of testosterone for short periods do not result in advancement of bone age or development of pubic hair. Whether testosterone replacement should be performed during the first 6 months of life to mimic the neonatal activation of the gonadal axis is unclear; in any case, replacement would better be done with gonadotropins to promote testicular effects (Bouvattier et al., 2012; Young et al., 2019).
Percutaneous treatment has been described in infants and children with micropenis: For 30 days, 10 mg (0.2 g of 5% testosterone cream) applied daily onto the phallus at night resulted in a significant increase of approximately 9 mm in penile length without changes in bone age (Arisaka et al., 2001).
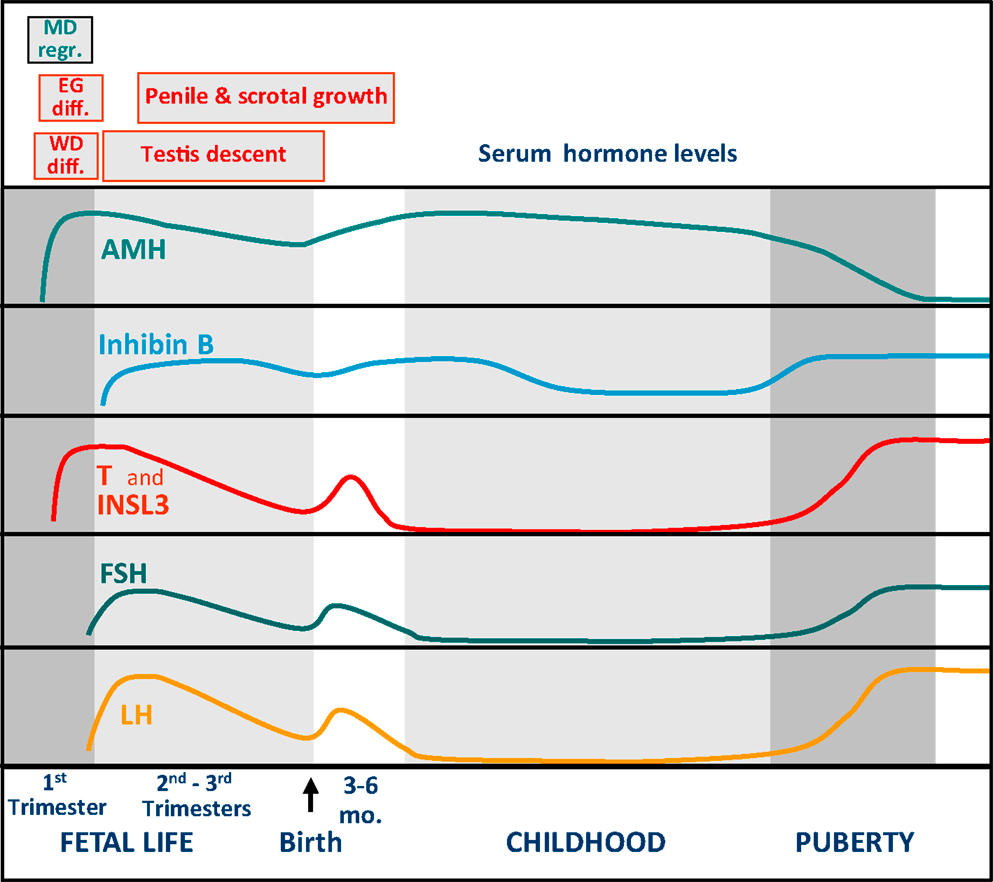
In early fetal development, the testis secretes –independently of pituitary gonadotropins– androgens and anti-Müllerian hormone (AMH) which are essential for...
www.frontiersin.org
In early fetal development, the testis secretes – independent of pituitary gonadotropins – androgens and anti-Müllerian hormone (AMH) that are essential for male sex differentiation. In the second half of fetal life, the hypothalamic–pituitary axis gains control of testicular hormone secretion. Follicle-stimulating hormone (FSH) controls Sertoli cell proliferation, responsible for testis volume increase and AMH and inhibin B secretion, whereas luteinizing hormone (LH) regulates Leydig cell androgen and INSL3 secretion, involved in the growth and trophism of male external genitalia and in testis descent.This differential regulation of testicular function between early and late fetal periods underlies the distinct clinical presentations of fetal-onset hypogonadism in the newborn male:primary hypogonadism results in ambiguous or female genitalia when early fetal-onset, whereas it becomes clinically undistinguishable from central hypogonadism when established later in fetal life. The assessment of the hypothalamic–pituitary–gonadal axis in male has classically relied on the measurement of gonadotropin and testosterone levels in serum. These hormone levels normally decline 3–6 months after birth, thus constraining the clinical evaluation window for diagnosing male hypogonadism. The advent of new markers of gonadal function has spread this clinical window beyond the first 6 months of life.In this review, we discuss the advantages and limitations of old and new markers used for the functional assessment of the hypothalamic–pituitary–testicular axis in boys suspected of fetal-onset hypogonadism.
The concept of male hypogonadism is usually associated with the adult patient, and rarely thought of as a condition in the prepubertal boy. Furthermore, male hypogonadism is most frequently equated to hypoandrogenism. Androgens are the dean of testicular hormones, and the normal testis produces very little or no testosterone during most of infancy and childhood. It is therefore easy to understand why the term hypogonadism is almost absent from the pediatrician’s terminology. However, many hypogonadal states in the male bear their origin in fetal life. With the advent of direct markers of Sertoli cell function, hypogonadism can be identified in boys beyond the early post-natal critical window of pituitary–gonadal activation (1) – called “mini-puberty” by some authors – and before pubertal age.In this review, we address the diagnostic approaches of fetal-onset male hypogonadism based on the physiology and pathophysiology of the hypothalamic–pituitary–testicular axis ontogeny.
Concluding Remarks
Fetal hypogonadism of the first trimester is primary and results in dysgenetic or cell-specific forms of DSD. In the second and third trimesters, primary and central hypogonadism share signs of hypoandrogenism and defective INSL secretion – i.e., micropenis, hypoplastic scrotum and cryptorchidism – and of Sertoli cell hypoplasia – i.e., microorchidism. In prepubertal patients, classical serum markers, like gonadotropins and testosterone, are helpful essentially during the first 3–6 months of life. With the advent of AMH and inhibin B, a biochemical diagnosis can also be envisaged during the rest of childhood. Clinical findings may also help in the diagnosis beyond early infancy. Finally, the pediatrician should not expect elevated gonadotropin levels during childhood to foresee a primary hypogonadism.


.webp")