Castaneda
Member
This will be my first post here.
I have suffered symptoms of low T for quite some time, and I have been consulting with various hormone experts trying to understand my steroid hormone metabolism more deeply. I won't name names, but I keep hearing "there is nothing you can do about this, and you need TRT". I haven't jumped to that conclusion yet. Let me explain why:
I have done several tests, with and without precursors like DHEA and Pregnenolone. Without them, Life Extension labs show the following values (we'll call this my baseline):
Testosterone, Serum 672 ng/dL (264-916)
Free Testosterone (Direct) 9.9 pg/mL (6.8-21.5)
DHT 55 ng/DL (30-85)
LH 3.0 mIU/mL (1.7-8.6)
FSH 2.5 mIU/mL (1.5-12.4)
DHEA-S 186.6 ug/dL (102.6-416.3)
Estradiol 9.5 pg/mL (7.6-42.6)
Estrogens, Total 115 pg/mL (40-115)
SHBG 88.6 nmol/L (16.5-55.9)
I read this to mean my testosterone and especially E2 are low because of insufficient DHEA (possible adrenal stress). What has me puzzled are the total estrogens (top of range) and extremely high SHBG. We know that SHBG goes up, generally, under two circumstances: high estrogen and high thyroid hormones. The latter is not a problem (with high RT3 and lower than optimal T3, 25.2 and 2.9, respectively). TSH is 3.1 (I know). So that leaves me to believe SHBG is going up because of high estrone.
I have tried to fix this problem by taking extra DHEA, but it just exacerbates the problem. The more DHEA, the more estrone goes up and T and E2 remain more or less the same. I have also tried Pregnenolone and DHEA together, and while this does seem to raise T and E2, E1 continues to overflow like a waterfall. DIM just lowers E2 further, creating symptoms.
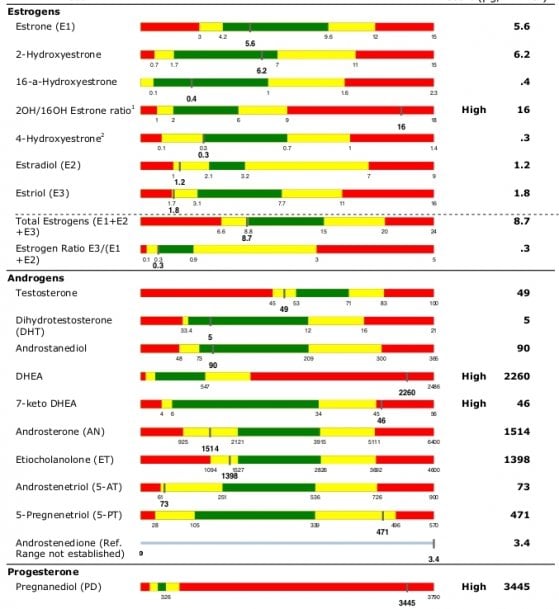
Not long ago, I decided to try Pregnenolone only at ~10mg, 3x a day and then did a 24-hour urine Rhein Lab metabolite panel (attached). You will see moderately low T and E2 (as espected), in range E1, extremely high 2OH/16OH ratio (also not surprising) and DHEA totally off the charts at 2260. Pregnanediol is also extraordinarily high, but that's typical with Preg.
No matter what I do, my body just wants to take DHEA and aromatize it to E1 (via Androstenedione), with T and E2 suffering. I keep coming back to poor 17-beta HSD expression. The other thought I had, and my reason for posting here, is... could it be that because DHEA is aromatizing to heavily ot E1 that it is bringing up SHBG and, in turn, binding to T and E2, pushing them down? In other words --- E1 is going out of control, liver pumps out SHBG to handle it, and it ends up taking otherwise good T / E2 levels with it.
That last idea was behind my last experiment inspired from a few posts over on the Ray Peat forum. I decided to try putting a 5mg/5mg solution of Pregnenolone and DHEA directly on the scrotum two times a day in combination with 5mg of Androsterone (which is supposedly able to inhibit aromatase with 90% efficiency). That's a total of 10mg Preg, 10mg DHEA and 10mg Androsterone per day. Initially, I felt quite well, but about a week into it, I started getting tendonitis and muscle aches to the point of feeling like an old man. Just a guess: androsterone was probably bringing down estrone but, again ... E2 coming too low as well. That's nearly as dangerous as high E2.
Regardless, libido, motivation, and energy are in the toilet, no matter what I do.
The last doc I spoke to said the only way to overcome that high SHBG is directly with testosterone gel. I'm not opposed to the idea, but I want to get some additional input from the forum here to see if anyone else has seen this pattern (before I go off and shrink my testicles to peanuts). When you inhibit aromatase, it's rather indiscriminate (as far as I understand). You are pulling back the reigns on both Androstenedione > Estrone and Testosterone > E2. The former is the problem, me probably needing more of the latter.
If I were to take just straight HCG, that would bypass the whole DHEA conversion problem, but my DHEA without any precursors was low, as shown on the LE lab above. It's a real Catch 22 and I can't help but think I'm missing something here.
Any ideas?
I have suffered symptoms of low T for quite some time, and I have been consulting with various hormone experts trying to understand my steroid hormone metabolism more deeply. I won't name names, but I keep hearing "there is nothing you can do about this, and you need TRT". I haven't jumped to that conclusion yet. Let me explain why:
I have done several tests, with and without precursors like DHEA and Pregnenolone. Without them, Life Extension labs show the following values (we'll call this my baseline):
Testosterone, Serum 672 ng/dL (264-916)
Free Testosterone (Direct) 9.9 pg/mL (6.8-21.5)
DHT 55 ng/DL (30-85)
LH 3.0 mIU/mL (1.7-8.6)
FSH 2.5 mIU/mL (1.5-12.4)
DHEA-S 186.6 ug/dL (102.6-416.3)
Estradiol 9.5 pg/mL (7.6-42.6)
Estrogens, Total 115 pg/mL (40-115)
SHBG 88.6 nmol/L (16.5-55.9)
I read this to mean my testosterone and especially E2 are low because of insufficient DHEA (possible adrenal stress). What has me puzzled are the total estrogens (top of range) and extremely high SHBG. We know that SHBG goes up, generally, under two circumstances: high estrogen and high thyroid hormones. The latter is not a problem (with high RT3 and lower than optimal T3, 25.2 and 2.9, respectively). TSH is 3.1 (I know). So that leaves me to believe SHBG is going up because of high estrone.
I have tried to fix this problem by taking extra DHEA, but it just exacerbates the problem. The more DHEA, the more estrone goes up and T and E2 remain more or less the same. I have also tried Pregnenolone and DHEA together, and while this does seem to raise T and E2, E1 continues to overflow like a waterfall. DIM just lowers E2 further, creating symptoms.
Not long ago, I decided to try Pregnenolone only at ~10mg, 3x a day and then did a 24-hour urine Rhein Lab metabolite panel (attached). You will see moderately low T and E2 (as espected), in range E1, extremely high 2OH/16OH ratio (also not surprising) and DHEA totally off the charts at 2260. Pregnanediol is also extraordinarily high, but that's typical with Preg.
No matter what I do, my body just wants to take DHEA and aromatize it to E1 (via Androstenedione), with T and E2 suffering. I keep coming back to poor 17-beta HSD expression. The other thought I had, and my reason for posting here, is... could it be that because DHEA is aromatizing to heavily ot E1 that it is bringing up SHBG and, in turn, binding to T and E2, pushing them down? In other words --- E1 is going out of control, liver pumps out SHBG to handle it, and it ends up taking otherwise good T / E2 levels with it.
That last idea was behind my last experiment inspired from a few posts over on the Ray Peat forum. I decided to try putting a 5mg/5mg solution of Pregnenolone and DHEA directly on the scrotum two times a day in combination with 5mg of Androsterone (which is supposedly able to inhibit aromatase with 90% efficiency). That's a total of 10mg Preg, 10mg DHEA and 10mg Androsterone per day. Initially, I felt quite well, but about a week into it, I started getting tendonitis and muscle aches to the point of feeling like an old man. Just a guess: androsterone was probably bringing down estrone but, again ... E2 coming too low as well. That's nearly as dangerous as high E2.
Regardless, libido, motivation, and energy are in the toilet, no matter what I do.
The last doc I spoke to said the only way to overcome that high SHBG is directly with testosterone gel. I'm not opposed to the idea, but I want to get some additional input from the forum here to see if anyone else has seen this pattern (before I go off and shrink my testicles to peanuts). When you inhibit aromatase, it's rather indiscriminate (as far as I understand). You are pulling back the reigns on both Androstenedione > Estrone and Testosterone > E2. The former is the problem, me probably needing more of the latter.
If I were to take just straight HCG, that would bypass the whole DHEA conversion problem, but my DHEA without any precursors was low, as shown on the LE lab above. It's a real Catch 22 and I can't help but think I'm missing something here.
Any ideas?