Nelson Vergel
Founder, ExcelMale.com

From the book: Testosterone: A Man's Guide
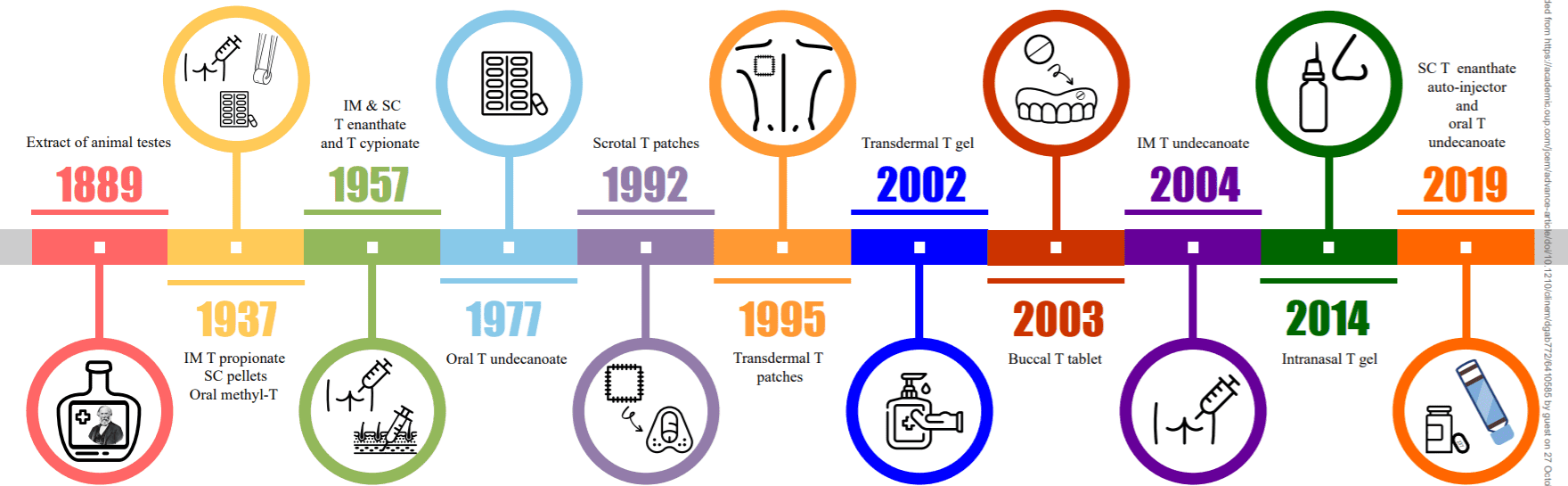
Testosterone Formulations
In theory, testosterone replacement should approximate the body's own natural production of the hormone. The average male produces 4 to 7 mg of testosterone a day with higher plasma levels in the early morning and lower levels in the evening. Women produce around a 12th of those rates.
Testosterone replacement is usually a lifelong commitment. It is a decision that should not be made without a discussion with your healthcare provider. Starting and stopping testosterone can have negative effects on someone's quality of life (more on this topic later).
There are testosterone replacement products that require daily dosing (orals, buccal, and gels), once a week or two weeks dosing (injections), and once every three- to four-month dosing (long-acting testosterone undecanoate injections or testosterone pellets).
Males who are hypogonadal can be given continuous testosterone replacement therapy in a wide assortment of ways. These include:
1. Oral capsules
2. Testosterone Injections
3. Transdermal (absorbed through the skin) testosterone cream or gel
4. Transdermal testosterone patch
5. Buccal (sublingual and gum adherent)
6. Pellets (that are implanted subcutaneously)
Oral Agents
Oral testosterone formulations are quickly absorbed by the liver and therefore require relatively large doses. Because of the risk of liver toxicity they are rarely prescribed. Do not waste your money or time using oral testosterone. Also, avoid over-the-counter supplements that claim to increase testosterone. Most do not increase testosterone for more than a few minutes and can also affect your liver and blood pressure. Oral testosterone also seems to cause larger decreases in good cholesterol (HDL) than other forms of testosterone therapies.
Chemically unbound testosterone, if taken orally, is immediately deactivated by the liver. Two chemically modified forms of testosterone are available that require several doses a day: methyltestosterone and testosterone undecanoate (not approved in the United States but popular in Canada).
Methyltestosterone
Methyltestosterone is one of the earliest available oral testosterones. Its chemical structure is the hormone testosterone with an added methyl group at the c-17 alpha position of the molecule to slow down its clearance by the liver. The use of oral c-17 alpha methylated testosterone causes toxicity to the liver and is not recommended for testosterone hormone therapy. Brand names around the world include “Metesto,” “Methitest,” “Testred,” “Oreton Methyl,” and “Android.” These products are responsible for many of the misconceptions that still exist about testosterone replacement due to their liver and lipid problems. The same information is applicable to fluoxymesterone, another oral formulation no longer used in the United States.
Testosterone undecanoate
Testosterone undecanoate is not a c-17 alpha alkylated hormone. Therefore it is considered a safer oral form of testosterone. It is designed to be absorbed through the small intestine into the lymphatic system and has fewer negative effects on the liver. Brand names around the world for oral testosterone undecanoate include “Andriol,” “Androxon,” “Understor,” “Restandol,” and “Restinsol.” It is not available in the United States but widely used in Canada and some European countries.
Jatenzo is the oral testosterone undecanoate approved in the US.

Jatenzo: An Advancement in Oral TRT
https://reachmd.com/programs/medical-industry-feature/advancement-oral-testosterone-replacement-therapy/11577/?autoplay=video Join Dr. Jennifer Caudle as she welcomes Dr. Adrian Dobs and Dr. Faysal Yafi to discuss testosterone replacement therapy and an oral soft gel option for appropriate...
One disadvantage of orally administered undecanoate is that it is eliminated from the body very quickly, usually within three to four hours. Frequent administration is necessary—usually from three to six capsules a day, which makes it impractical for most men with busy lives.
DITEST™- Oral Native Testosterone
https://www.diurnal.com/Investor/news/successful-outcome-of-oral-testosterone-clinical-study DITEST™ In addition to its hydrocortisone products, Diurnal’s is also developing a novel formulation of testosterone for the treatment of hypogonadism. Male hypogonadism is defined as testosterone...
Tlando: Another Oral Testosterone Undecanoate OK'd for Hypogonadism
FDA approval of Tlando follows in the footsteps of Jatenzo The recommended dosage is 225 mg orally twice daily with food. It does not require dose titration. "We believe Tlando's oral formulation and convenient dosing, which requires no titration, differentiates it from other treatment...
FDA Approves Oral Testosterone Replacement Therapy Kyzatrex
Another oral testosterone undecanoate. https://www.empr.com/home/news/fda-approves-oral-testosterone-replacement-therapy-kyzatrex/
Oral TRT Products: Jatenzo, Tlando, Kyzatrex, & DiTest
Testosterone Replacement Therapy: A Narrative Review with a Focus on New Oral Formulations (2022) Salman Z Bhat and Adrian S Dobs Male hypogonadism affects 10–30% of the male population and is often under-recognized and under-treated. Different replacement formulations exist, each with...
Intramuscular Injections
The most common testosterone replacement used by men worldwide is intramuscular testosterone injection. It's also the oldest and most economical way to increase blood levels of testosterone. This most cost-effective option is usually covered by insurance programs and community clinics.
The two most common esters, testosterone cypionate, and testosterone enanthate, are both generic medications in the United States. They are given at a weekly dose of about 100 to 200 mg a week (or 200 to 300 mg every two weeks).
Currently, a 10 ml bottle of 200 mg/ml (2000 total milligrams per bottle) of testosterone cypionate obtained in U.S. pharmacies cost around $85-$115. The cost of the same strength and amount of testosterone cypionate costs $33- $50 from compounding pharmacies. It is the same product, so if your insurance company does not pay for testosterone, make sure that you use compounding pharmacies. More information on compounding will be provided later.
Some physicians have patients come to their office for injections and others empower their patients to do so at home. A minority of physicians charges a fee for the office visit when you come for an injection, which can increase your costs.
When you get a prescription for any testosterone ester, make sure that it is for a 10-ml vial, not 1-ml vial. In the U.S., 1-ml vials are available but they are usually more expensive and not very practical. Many physicians will write an open-ended prescription that will look like this:
1. Testosterone Cypionate (or Depo-Testosterone), 10 ml, 200mg/ml, #1,
as directed, 1 refill
Others will write:
2. Testosterone Cypionate, 10 ml, 200 mg/ml, #1, 200 mg q 2 weeks, 1
refill
Or
3. Testosterone Cypionate , 10 ml, 200 mg/ml #1, 100 mg q 1 week, 1
refill
Be sure your physician gives you a more flexible prescription that reads like my first example. This type of prescription will provide room for you to adjust the dosage during the first two months as well as get a refill whenever you need it.
Optimum testosterone doses can range from 100 mg to 250 mg a week but it is practically impossible to predict an individual's response. Giving yourself a little room for adjustment keeps you from running out of testosterone if your insurance company denies your next refill because they think it's too early. Of course, your physician has to ensure that your dose is adjusted based on your total or free testosterone blood levels.
When using injectable testosterone, your doctor will want to measure your total blood testosterone levels right before your next injection after the first month (it takes a while for the blood levels to stabilize). If testosterone is >900 ng/dl (24.5 nmol/liter) or < 500 ng/dl, adjust dose or frequency. Anecdotally, most men seem to need to have total testosterone levels above 500 ng/dl (midpoint of normal range) to experience any of the expected sexual function benefits.
A dose for women is anywhere from 2.4 to 20 mg/week but because it is difficult to inject such low doses and because of the risk of masculinization (growth or facial hair, deepening of the voice, and growth of clitoris), many doctors prefer low dose creams to treat women. Compounding pharmacies like Women's International Pharmacy can guide doctors on how to test and prescribe testosterone gels to women. Their website is womensinternational.com. They have an excellent information packet that they send to people for free that contains several research papers and protocols for women.
There is no commercially available FDA-approved testosterone therapy for women in the United States as of 2011, but one option may be approved in 2012 (Libigel, mentioned later). However, many doctors can legally prescribe testosterone to women in an off-label manner using compounded gels and creams. However, some doctors are reluctant to prescribe any hormones to women since the discouraging results from female hormone replacement in women showed increased cardiovascular risk in women.
Injections have the advantage of once-per-week (or every two weeks) administration, so it may be a more acceptable option for men who do not want to deal with the daily administration typically needed with gels. However, there are concerns about their “peak-and-valleys” testosterone blood level patterns.
The standard dose of 200 mg testosterone injections currently used in the United States produces unnaturally high blood testosterone and estradiol levels during the initial few days after injection. Then the blood level drops off each day and falls to baseline in about 10 days. This method does not effectively deliver sustained normal blood levels of testosterone or mimic the natural daily pattern of testosterone release as well as other treatment options. There is a concern that some men using 200 mg of testosterone cypionate every two weeks may have low levels of testosterone by day 10, so they spend four days with low testosterone before their next injection. For this reason, I have seen that a dose of 100 mg of testosterone cypionate or enanthate weekly is becoming more and more commonly prescribed by doctors who treat a lot of hypogonadal men.
Your doctor should re-check your testosterone level after one month (after steady state occurs) right before the next injection. This testing schedule allows him to see whether normal levels are still present when you reach your lowest testosterone blood level. If serum total testosterone level is more than 900 ng/dL or less than 500 ng/dL right before the next dose, he /she can adjust the dose or the frequency accordingly.
Due to testosterone's effect as a stimulant of red blood cell production, injections produce unusually strong stimulation during the first peak days. This appears to increase the potential for elevated hemoglobin and hematocrit indicating that you have too many red blood cells. These can increase your cardiovascular risks. Creams, gels, and patches appear to be less likely to produce this side effect, though study results are conflicting.
Anecdotally I hear that injections promote elevations in blood pressure more than creams, gel, and patches. It also appears that the effect on brain chemistry and the nervous system that might promote increased assertiveness can be stronger with injections. There will be more discussion on this subject later. But I would love to see head-to-head comparison studies between testosterone injections and gels since none have been performed to date. Hopefully, with the potential approval of Aveed (a longer acting testosterone ester) in the future, its manufacturer would be compelled to do such a study to convince insurance companies that their product may be more cost-effective and less problematic than the daily gels currently approved in the United States (Androgel and Testim) or the weekly or bi-weekly injections that many men are currently using.
I have met some men that have switched from injections to gels and then eventually switch back to injections. It seems that they need a higher level of overall metabolic stimulation that injectable testosterone provides. Usually, those men also say they feel very little improvement with the use of gels or creams. They also usually prefer the convenience of an injection every one or two weeks to the daily administration of a gel. And, unlike gels, injections have no potential risk of transferring testosterone through skin contact with other people.
Injectable testosterone has also shown to increase blood levels of testosterone and DHT in proportion with the dose. But gels seem to increase DHT a lot more than the expected increase due to higher testosterone, so some men with benign prostatic inflammation may prefer injections than gels. The mechanism for this observation may be based on the fact that they may be more DHT receptors in the skin layers, but no one has really proven this fact.
As you can see, there is no one-size-fits-all approach that works for everyone. Blank statements about one option being better than others have to be done in the context of other factors that go beyond the obvious. Convenience, doctor's prescription habits, personal lifestyle, cost, and what your insurance company pays are factors that determine what you use.
It is important to follow a strict injection procedure (for helpful tips, see the section on How to Inject Testosterone Safely). Some men report soreness in the injection area and experience coughing spells after injecting. In rare cases, some men have had infections in the injection site due to unsanitary techniques!
Commonly Used Injectable Esters for Testosterone Replacement Therapy
Testosterone esters are modifications made to the testosterone molecule to increase the time the liver breaks it down so that you do not have to inject every day. Esters consist of the actual testosterone molecule, with a carbon chain attached to it. This carbon chain controls something called the partition coefficient, which translates into how soluble the drug will be once in the bloodstream. Also, the larger the carbon chain, the longer the ester, the less soluble the drug is in water, and the longer it stays in your body. Also, additions to the basic testosterone molecule make it harder for the liver to break it down, which also increases the time testosterone stays in your system (a good thing since we do not want to deal with injections too frequently).
There are several types of testosterone esters: testosterone cypionate, enanthate, propionate, or undecanoate. Outside the United States, there is a product with a combination of the first three esters that is called Sustanon 250 (250 mg of a mixture of cypionate, enanthate, and propionate). Since every ester may have slightly different blood level decay after administration, it is speculated that this combination may allow better distribution of testosterone blood levels in 14 days. Sustanon is not available in the United States but compounding pharmacies may customize similar formulations.
Testosterone cypionate, enanthate, or other ester is injected slowly into the muscle of the buttock where it forms a reservoir of the hormone. Then testosterone is gradually released from the reservoir into the bloodstream. There is usually a peak concentration in the blood within the first two days and then a gradual decrease to baseline. Everyone is different and the rate of decrease in blood levels tends to change depending on body weight, fat content, activity level, medications, illness, and liver metabolism.
Testosterone Enanthate
Testosterone enanthate is one of the main forms of testosterone prescribed to men in the United States. It is a slow-acting ester, with a release time between 8 and 10 days. The name brand of testosterone enanthate available in the United States is called “Delatestryl,” which is suspended in sesame oil. Testosterone enanthate is typically injected once every week to once every two weeks. Generic testosterone enanthate can also be obtained through a compounding pharmacy; such pharmacies can mix the enanthate in either sesame, grapeseed or cottonseed oil. Some mix different esters for patients since this may give better blood level distribution, although no studies have been done in the United States using ester blends.
For more details about this product, refer to the Appendix section for the package insert. Package inserts are required by the FDA to be provided with every product when you pick it up at the pharmacy. They are also required when magazine ads or promotional materials are provided on products. That is why I thought it would be a good idea to include a package insert on an injectable and a gel at the end of this book. Every patient should read package inserts of every medication they take but keeping in mind that a lot of the side effects listed are not common and only happen in special circumstances. But it does not hurt to know them just in case!
Testosterone cypionate
Testosterone cypionate is the other main injectable form of testosterone prescribed to men in the United States. It is a slow-acting ester with a release time of 8 to 10 days, similar to that of enanthate. The name brand available in the United States is called “Depo-Testosterone,” which is suspended in cottonseed oil. Testosterone cypionate is typically injected anywhere from once every week to once every two weeks. Some doctors like to prescribe 300 mg every three weeks, but I believe that really accentuates the peaks and valleys of testosterone blood levels a lot more than the most commonly used dose of 200 mg every two weeks. Cheaper generic testosterone cypionate can also be obtained through a compounding pharmacy which can mix it in either sesame, grapeseed or cottonseed oil.
Sustanon 100 or 250
“Sustanon” is the brand name for two formulas of injectable testosterone that contain a blend of esters. “Sustanon 100” contains 100 mg of three testosterone esters: testosterone propionate, testosterone phenylpropionate, and testosterone isocaproate. “Sustanon 250” contains a total of 250 mg of four testosterone esters: testosterone propionate, testosterone phenylpropionate, testosterone isocaproate, and testosterone decanoate. Both formulas feature fast-acting and slow-acting esters and can be injected anywhere from once every week to once every four weeks. Sustanon is prescribed outside the United States, but a formulation similar to it can be compounded legally by compounding pharmacies since all of its esters are available in the United States.
Other Injectable Esters of Testosterone
Testosterone propionate
Testosterone propionate is a fast-acting ester with a release time of three to four days. To keep blood levels from fluctuating greatly, propionate is usually injected from one to three times a week. It is for this reason that it is not usually prescribed that much. Some users also report that propionate is a more painful injection, with swelling and noticeable pain around the injection site.
Testosterone phenylpropionate
Testosterone phenylpropionate is a slow-acting ester, with a release time of one to three weeks. A popular name brand for T-phenyl propionate is “Testolent.” Testosterone phenylpropionate is also one of the components of Sustanon.
Testosterone Undecanoate
Testosterone undecanoate injections are known as the brand name Nebido around the world. In the United States, it is called Aveed. This ester may stay longer in your system so that less frequent injections may be needed. The injection is usually given once every 10 to 14 weeks, though the frequency will depend on your individual testosterone levels. After your first injection, you may be asked to come back for another injection at week six. For use in the United States, the company claims that only five injections a year are needed (compared to 48 injections per year for a 100 mg per week regimen). In other countries, a large injection dose of 1000 mg is allowed. The FDA did not allow the manufacturer to use this dose in studies done in this country due to fears of side effects. More information on Aveed
In an open-label study which enrolled 130 hypogonadal men with blood total testosterone levels below 300 ng/dL at study entry, Aveed was dosed as an intramuscular injection (750 mg) at baseline, at week four, and then every 10 weeks throughout the remainder of the 21-month study. Approximately 70 percent of patients completed all injections and 94 percent of them had total testosterone from 300 to 1,000 nanograms/ml through the entire study.
After Nebido was approved in Europe a small number of European patients experienced respiratory symptoms immediately following intramuscular injection of 1000 mg in a 4 cc injection volume, (versus the 750 mg, 3 cc injection volume used in the United States). The makers of Nebido believe, and the FDA concurs, that the reaction is likely the result of a small amount of the oily solution immediately entering the vascular system from the injection site. This known yet uncommon complication of oil-based depot injections may be related to inappropriate injection technique or site.
The problem is characterized by short-term reactions involving an urge to cough or shortness of breath. In some rare cases, the reaction had been classified as serious or the patient had experienced other symptoms such as dizziness, flushing or fainting. In U.S. clinical trials of Nebido 750 mg (3 cc injection volume), the proposed dose in the U.S., there was a single, mild, non-serious case of oil-based coughing.
PERSONAL COMMENT: I have used testosterone enanthate, cypionate, and Sustanon 250. I cannot say I can tell the difference in the way I felt. I also tried one injection of Nebido in Mexico. After a big injection of the recommended dose of 1,000 mg, my testosterone blood levels remained above 450 ng/ml for four and a half months; my mood and stamina remained very good throughout. It was nice not having to worry about remembering to inject every week.
More on testosterone esters
Testosterone Cypionate vs Enanthate : Formulation Differences
Testosterone Oils: Cottonseed vs Sesame Seed Oils
Transdermal Systems
Transdermal gels (Androgel, Testim)
Creams and gels may provide lower and more sustained concentrations of testosterone in the blood without the “yo-yo” effect that weekly injections can cause. Testosterone gets absorbed through the skin once or twice daily use.
The best application areas for the gel include the stomach, shoulders, the inner thighs, and the pectorals. Be aware that some people complain about dark hair growth where the cream or gel is applied, especially if one site is used over and over again without rotation.
As mentioned if you use testosterone this way, it can rub off onto a female partner or children when you hug them. So, it is important that this is kept in mind.
I think that its application on the back of the legs may help avoid this potential transfer of testosterone to other people. Most testosterone in gels and creams gets absorbed in the first one to two hours, but some residual testosterone may still be present after a few hours.
Topical testosterone products represent approximately 65.6 percent of the total number of testosterone prescriptions dispensed between 2000 and November 2008, according to the FDA. Two prescription-based commercial testosterone gels are available in the United States: Androgel, approved by the FDA in February 2000, and Testim, approved in October 2002 (See Figure 11). Approximately 1.4 million prescriptions were dispensed for Androgel and 400,000 prescriptions were dispensed for Testim in 2008. The majority of prescriptions for Androgel are dispensed to adult males 50 to 59 years of age.
Both gels are colorless and evaporate quickly after being applied to the abdomen, shoulders, or arms. Androgel and Testim come in three dose levels (2.5 g, 5 g and 10 g with 1 percent testosterone each). Ten percent of the applied testosterone is absorbed into the bloodstream through the skin. The usual starting dose is a packet of 5 g a day.
Androgel also comes in a pump that allows for higher dosing for those men who do not reach normal testosterone levels with the available gels. Each pump container is capable of dispensing 75 grams or 60 metered 1.25- gram doses. The starting dose of 5 grams a day requires four pump squirts. Many men require up to 10 grams per day to reach total testosterone blood levels above 500 ng/ml. This makes for eight squirts a day of Androgel. For some, that is a lot of volume to spread on the body. Luckily these gels dry up fast and leave little to no residue.
Auxilium, the maker of Testim, claims that their gel has a slightly better absorption rate than Androgel; however, many men do not like its slight soapy smell (Androgel has none).
Androgel and Testim are usually covered by insurance. Their monthly cost is around US$700 a month, with insurance co-pays ranging from US$20 to US$50 a month. A patient assistance program has been set up by both companies to provide free drug to low-income patients with no insurance (read the resource section in this book for additional information).
At the time of writing this book, some companies were getting ready to manufacture generic testosterone gels which may provide a cheaper alternative.
Regardless of which gel you use, make sure your doctor re-checks your blood levels after two weeks to see whether you need to readjust the dose.
Testosterone gels should be applied to clean, dry skin. Do not apply to the testicular area since this has been shown to increase DHT conversion.
Application sites should be allowed to dry for a few minutes before dressing. Hands should be washed thoroughly with soap and water after application. In order to prevent transfer of testosterone to another person, clothing should be worn to cover the application sites. If direct skin-to-skin contact with another person is anticipated, the application sites should be washed thoroughly with soap and water. Users should wait at least two hours after applying before showering or swimming; for optimal absorption, it may be best to wait five to six hours.
Men who may carry babies should be extra careful to avoid skin-to-skin contact after applying the gel since testosterone exposure in babies may have negative effects on the baby's growth. This fact was included in a recent label change for both Testim and Androgel described in the FDA web site: “Since the initial marketing approval of testosterone gel in 2000 to May 2009, FDA's Adverse Event Reporting System (AERS) received 20 reports (18 U.S. and 2 non-U.S.) describing adverse events in children who were exposed to testosterone gel that was used by another person (referred to as ‘secondary exposure'). The adverse events reported in these children included one or more of the following signs or symptoms: enlargement of the penis or clitoris, premature development of pubic hair, advanced bone age, increased self-stimulation, libido, erections, and aggressive behavior. An increased testosterone level was reported in more than half of these cases. The children ranged in age from 9 months to 7 years. Three of the 20 cases are described in the medical literature.” So, be careful not to come in contact with another person during the first 4 hours of administration.
Compounded creams and gels
Compounded creams and gels can be mixed by compounding pharmacies, and are similar in dosing, application, and precautions to what is described above for Androgel and Testim. There are various qualities of creams and gels made by compounding pharmacies around the United States, and some of the poorer quality products are gunky and flake off after they dry. Be sure to buy from a reputable pharmacy.
The best gels are clear and basically disappear shortly after application. Most men prefer alcohol-based gels, which absorb through the skin better than water-based gels. Creams should not be greasy and should resemble good moisturizing creams. Many compounding pharmacies make cheaper gels and creams with higher testosterone concentrations (2 to 10 percent) for men who do not respond to the commercially available 1 percent testosterone gel products (Testim or Androgel).
Some doctors do not feel comfortable prescribing gels from compounding pharmacies since they worry about quality control. There is also concern that higher concentration gels may induce more DHT conversion, which may cause more prostatic hyperplasia (inflammation) causing urinary flow restrictions, especially in older men. Also, higher DHT can cause acne and hair loss.
There are many compounding pharmacies around the United States. I have used several compounding pharmacies in the past 15 years.
You can also Google the keywords: “compounding pharmacy” and your zip code to find compounding pharmacies close to you. Compounding pharmacies ship across state lines, so it is not imperative that you have one in your area. They do not typically take insurance, so you have to request reimbursement from your insurance company. Your doctor has to be willing to call or fax a prescription to the pharmacy for you to order any testosterone products. The compounding pharmacy will need your credit card before shipping the product to you, so make sure you call them to set that up.
Most compounded testosterone gels of 1 to 10 percent concentrations can range between $17 and $70 a month so it's worth calling around for price comparisons. Your doctor may have an established relationship with a local compounding pharmacy, so be sure to ask. As mentioned before, some doctors have trust issues with compounding pharmacies' quality control and ask to see their certificates to prove that they have proper quality control standards.
There are two main advantages of using compounding pharmacies when getting a testosterone gel or cream. The first is cost: until a generic version of the gel is available, compounded gel will usually be the cheaper alternative. This is a non-issue if you have an insurance policy that pays for the product and that it does not require you to pay high out of pocket co-pays when getting Androgel, Testim, Fortesta or Axiron.
The second is customization: your doctor can write a prescription of varying concentration for gels or creams. I have used gels containing 5 and 10 percent testosterone with great results. Of course, the volume needed is lower when the concentration increases. Some researchers believe that higher concentration gels tend to increase DHT levels more strongly than the regular 1 percent gels. However many men need more than the usual amount of Testim or Androgel and do not want to smear their bodies with lots of gel, so 5 percent gels may be an option for them.
Most compounding pharmacies dispense the creams in “Topi-Click” (see Figure 13) that are more practical (typically) than the large preloaded syringes they are usually supplied in. The Topi-Click is more like a “deodorant stick” which can be more convenient and better looking than the bigger syringes.
Testosterone in Atrevis hydrogel base = almost double test levels!
So I was using 200 mg/gm compounded cream from Empower, which is HRT base, for almost 3 years before I switched to Medquest Pharmacy to try the Atrevis Base. I have heard about increased absorption from Atrevis base, but damn! I was using 3 clicks twice daily of Empower’s HRT base and never got...
Factors that Can Improve Testosterone Gel Absorption
Types of Transdermal Testosterone Products Currently Available
PERSONAL COMMENT: I tried both Androgel and Testim for a few weeks. Both were effective but I admit to having a little sticker shock ($260 to $600 per month depending on dose, if not paid by insurance). Testim had a soapy smell that I didn't particularly like, but some gave me compliments on my “cologne.” I did like the large pump dispenser for Androgel since I could adjust the dosage if needed (I needed 10 grams of gel a day. Most doctors start you at 5 grams per day). I am currently using a testosterone gel/cream formulation with 5 percent testosterone. The prescription is written like this: Testosterone gel/cream 5 percent 30 mL in Topi-Click, 1 mL a day. I find the Topi-Click container to be a very easy way to administer the daily dose. You can also order the gel in a large graduated plastic syringe if you want to precise on your dose.
More on transdermal testosterone products: Types of Transdermal Testosterone Products Currently Available
Transdermal patches
Another option for testosterone replacement therapy is a testosterone patch such as Testoderm or Androderm. For many men, two 5-mg patches will bring them into the effective mid-range (500 ng/dL and above) of the testosterone blood test. The most frequent complaint with the patch is skin irritation at the application site. Some men do not like the potential of an unwanted “disclosure” since the patch can be visible to anyone who may see you without clothes. You also run the risk of having the patch fall off after sweating or bathing.
Androderm
Androderm comes in two doses: A 2.5 mg/patch and a 5.0 mg/patch. The actual amount of testosterone in the 2.5 mg patch is really 12.2 mg, while in the 5.0 mg patch it is 24.3 mg. Similar to what happens with the gel, much of the testosterone in the patch will not be absorbed into your system. So the aim of the 2.5 mg patch is to get 2.5 mg of testosterone successfully into the bloodstream each day. It is possible to absorb slightly more or slightly less than the 2.5 mg patch's ideal dosage (this applies to the 5.0 mg patch as well). Most men need not one but two patches of 5 mg each to attain total testosterone blood levels above 500 ng/dL.
Androderm patches are usually applied on the back, abdomen, thighs, or upper arms. Because the active area of the patch is covered, you can enjoy some worry-free skin contact with your partner. As with any form of testosterone, your blood level will need to be checked by your doctor to readjust your dosage. Since dosages vary between 2.5 and 10 mg daily, this may require one or more patches.
It seems from the data that Androderm does not raise DHT or estrogen levels too much, so this may be an advantage for this option.
PERSONAL COMMENT: I have used Androderm and I have to say that I was not very fond of this product. I felt kind of exposed when I was naked, I didn't want to have to talk about testosterone replacement therapy just when things were getting interesting. Some countries and public clinics provide only Androderm as the only option for TRT; it is a good option I would not discourage anyone from using it.
Testoderm TTS
Testoderm was first introduced as a patch that you would have to apply to the scrotum (testicular sack) after shaving it. For obvious reasons, it was not very practical and discreet (imagine explaining to any sexual partners what that patch is doing there and that you are not injured as it may seem!). It also showed large increases in DHT since the scrotum tissue seems to facilitate the conversion of testosterone into DHT. For this reason, a new non-scrotal patch was developed. Testoderm TTS patches are available in two doses: 4.0 and 6.0 mg/patch. As with Androderm, the actual amount of testosterone in these patches is greater than the listed dose because much of the testosterone will not be absorbed.
Testoderm TTS patches are usually applied on the back, abdomen, thighs, or upper arms. Since the patch is covered ( like in the case of Androderm) you don't have to worry about transferring the testosterone through skin contact with a partner. Dosages will vary between 4.0 and 12 mg daily requiring one or more patches. Again, after a starting dose, your testosterone level will need to be re-checked by your doctor a month after to determine the right dose for you.
Anecdotally Testoderm TTS seems to increase DHT levels more than most other options in the market, although a study showed constant testosterone/DHT ratios, meaning that both values increased in the same proportion.
For information on testosterone patient assistance programs (Androgel, Testim, Fortesta, Axiron, testosterone cypionate): Click here
More testosterone options:
Testosterone Pellets, Sublingual and Buccal (Mouth)
Last edited: