
It was more a matter of continued experimentation. While on only enanthate I felt there was room for improvement and wanted to see what propionate would be like. When I saw the large variations in serum testosterone with daily propionate I started thinking about how to damp them down to more natural amplitudes. This is how I eventually arrived at the blend. Although there's utility in getting some numbers with single esters first, it's still possible to tune with a blend. You must either try to get peak and trough measurements or else make assumptions about your rate of absorption.@Cataceous, as you know, I am interested in following your logic. I am currently not on either ester. I was planning on starting both esters simultaneously. As I read your post above, however, it sounds like you did this one ester at a time until you started the blend. Was this by design or were you in a trial and error and eventually ended up with the blend?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Tips on how to blend propionate with enanthate (or cypionate)?
- Thread starter Willyt
- Start date
-
- Tags
- blend daily low dose propionate


See my post on page 2. In a nutshell, I had to discontinue my attempt at the blended protocol using Cyp + Prop @ 1.2:1 ratio due to water retention from the cypionate. It's a problem that I've experienced before with larger doses of cypionate.Been following this closely. Would love to hear how others are doing on a daily protocol (blend or no blend). Please share your experiences. @Willyt, still doing well?
I am back on Propionate-only at 8mg per day and doing pretty well although I would have preferred the blend. I am going put together some notes in the coming weeks on my experience trying to tame the wild mustang of low dose daily Prop.
I have the same question.has anybdy tried dosing prop twice a day out of curiosty
have never seen it mentioned before
It would be easy enough to try (surely someone has done so on this board). That is the beauty of low dose daily Prop. It clears out so fast that you can experiment with different protocols on a daily basis. For example, I can subjectively feel a small bump from 8mg to 9mg that same day. If you don't like the dose, switch back the following day.has anybdy tried dosing prop twice a day out of curiosty
have never seen it mentioned before
I see two challenges with 2x daily. First is compliance over a period of years. That second shot will be a major inconvenience for most people (including myself). The other issue is the timing of the second injection. Prop is known to energize. I would not want to inject too close to bedtime because Prop amps me up (think expresso after dinner). Then again, maybe you wouldn't feel a small 3-4mg dose as much?
I'll try it this weekend. How about 4mg @ 7am and 4mg @ 3pm so 8 hours between doses? Part of me hopes it doesn't work lol
Let us knowIt would be easy enough to try (surely someone has done so on this board). That is the beauty of low dose daily Prop. It clears out so fast that you can experiment with different protocols on a daily basis. For example, I can subjectively feel a small bump from 8mg to 9mg that same day. If you don't like the dose, switch back the following day.
I see two challenges with 2x daily. First is compliance over a period of years. That second shot will be a major inconvenience for most people (including myself). The other issue is the timing of the second injection. Prop is known to energize. I would not want to inject too close to bedtime because Prop amps me up (think expresso after dinner). Then again, maybe you wouldn't feel a small 3-4mg dose as much?
I'll try it this weekend. How about 4mg @ 7am and 4mg @ 3pm so 8 hours between doses? Part of me hopes it doesn't work lol
yea for sure the i would inject less in the evening as i find prop stimulatingIt would be easy enough to try (surely someone has done so on this board). That is the beauty of low dose daily Prop. It clears out so fast that you can experiment with different protocols on a daily basis. For example, I can subjectively feel a small bump from 8mg to 9mg that same day. If you don't like the dose, switch back the following day.
I see two challenges with 2x daily. First is compliance over a period of years. That second shot will be a major inconvenience for most people (including myself). The other issue is the timing of the second injection. Prop is known to energize. I would not want to inject too close to bedtime because Prop amps me up (think expresso after dinner). Then again, maybe you wouldn't feel a small 3-4mg dose as much?
I'll try it this weekend. How about 4mg @ 7am and 4mg @ 3pm so 8 hours between doses? Part of me hopes it doesn't work lol
madman
Super Moderator
It would be easy enough to try (surely someone has done so on this board). That is the beauty of low dose daily Prop. It clears out so fast that you can experiment with different protocols on a daily basis. For example, I can subjectively feel a small bump from 8mg to 9mg that same day. If you don't like the dose, switch back the following day.
I see two challenges with 2x daily. First is compliance over a period of years. That second shot will be a major inconvenience for most people (including myself). The other issue is the timing of the second injection. Prop is known to energize. I would not want to inject too close to bedtime because Prop amps me up (think expresso after dinner). Then again, maybe you wouldn't feel a small 3-4mg dose as much?
I'll try it this weekend. How about 4mg @ 7am and 4mg @ 3pm so 8 hours between doses? Part of me hopes it doesn't work lol
Need to keep in mind whether one is injecting cyp/enanthate/prop that post-injection there will be an initial burst release of T and levels will start rising within the first 2 hrs.
T levels will spike up fairly quickly even when using the medium-chain esters.
Enanthate has been shown to reach Tmax 10 hrs.
Even then when injecting prop T levels will not peak as fast as unesterified T suspension let alone Natesto!
See no point in injecting prop twice daily.
15.6.1 Testosterone propionate
Single-dose pharmacokinetics of 50 mg testosterone propionate after IM injection to seven hypogonadal patients, and the best-fit pharmacokinetic profile, are shown in Fig. 15.4 (Nieschlag et al. 1976). Maximal testosterone levels in the supraphysiological range were seen shortly after injection (40.2 nmol/l, Tmax = 14 h). Testosterone levels below the normal range were observed following day two (57 h) after injection. The calculated values were 1843 nmol·h/l for the area under the curve (AUC); 1.5 d for mean residence time (MRT); and 0.8 d for terminal half-life (Table 15.2).
Based on single-dose pharmacokinetic parameters, a multiple-dose pharmacokinetic simulation was performed. Expected testosterone serum concentrations after multiple dosing of 50 mg testosterone propionate, twice per week (e.g. injections Mondays and Thursdays, 8 a.m.), are shown in Fig. 15.5. Shortly after injection, high supraphysiological testosterone serum concentrations of up to 45 nmol/l are observed. At the end of the injection interval (three and four days, respectively), testosterone serum concentrations below the lower range of normal testosterone values are projected (7 nmol/l and 3 nmol/l, respectively).
15.6.4 Testosterone ester combinations
Testosterone ester mixtures have been widely used for substitution therapy of male hypogonadism (e.g. Testoviron® Depot 50: 20 mg testosterone propionate and 55 mg testosterone enanthate; Testoviron® Depot 100: 25 mg testosterone propionate and 110 mg testosterone enanthate; Sustanon® 250: 30 mg testosterone propionate, 60 mg testosterone phenylpropionate, 60 mg testosterone isocaproate, and 100 mg testosterone decanoate). These combinations are used following the postulate that the so-called short-acting testosterone ester (e.g. testosterone propionate) is the effective testosterone for substitution during the first days of treatment, and the so-called long-acting testosterone (e.g. testosterone enanthate) warrants effective substitution for the end of the injection interval. However, this assumption is not supported by the pharmacokinetic parameters of the individual testosterone esters. BOTH TESTOSTERONE PROPIONATE AND TESTOSTERONE ENANTHATE CAUSE THE HIGHEST TESTOSTERONE SERUM CONCENTRATIONS SHORTLY AFTER INJECTION (Fig. 15.4 and Fig. 15.6). Accordingly, the addition of testosterone propionate to testosterone enanthate only increases the INITIAL UNDESIRED TESTOSTERONE PEAK and worsens the pharmacokinetic profile that ideally should follow zero-order kinetics (Fig. 15.9). The computer simulation agrees well with the limited published single-dose testosterone values that have been measured in hypogonadal patients treated with the combination of testosterone propionate and testosterone enanthate. Maximal increases of approximately 40 nmol/l testosterone over basal values are described one day after IM administration of a testosterone ester combination
It's important to be aware that the measurements in this study were only once a day, at 8:00. The injection was at 18:00. So in reality Tmax could occur much sooner than 14 hours post-injection. My experience with propionate at low doses (<10 mg) is at least suggestive of a Tmax under six hours....
15.6.1 Testosterone propionate
Single-dose pharmacokinetics of 50 mg testosterone propionate after IM injection to seven hypogonadal patients, and the best-fit pharmacokinetic profile, are shown in Fig. 15.4 (Nieschlag et al. 1976). Maximal testosterone levels in the supraphysiological range were seen shortly after injection (40.2 nmol/l, Tmax = 14 h). ...
madman
Super Moderator
It's important to be aware that the measurements in this study were only once a day, at 8:00. The injection was at 18:00. So in reality Tmax could occur much sooner than 14 hours post-injection. My experience with propionate at low doses (<10 mg) is at least suggestive of a Tmax under six hours.
Indeed!
Bioavailability and LH-Suppressing Effect of Different Testosterone Preparations in Normal and Hypogonadal Men (1976)
Pharmacokinetic Properties of Testosterone Propionate in Normal Men (1986)
ABSTRACT
The pharmacokinetic characteristics of testosterone propionate were studied in normal men after a single IM dose of 25 mg testosterone propionate-19,i9,19-d3; Plasma levels of testosterone propionate-19,19,19-d3, its active metabolite testosterone-i9,19,19-d3, and endogenous testosterone were measured by gas chromatography-mass spectrometry. Testosterone propionate-19,19, l9-d3 was gradually transferred from the IM injection site to the systemic circulation. The plasma levels of testosterone propionate-19,l9,19-c<3 were maintained at 2-4 ng/ ml between 3 and 36 h after administration. Plasma testosterone-i9,19,19-d3 levels were maintained above the physiological testosterone level for 48 h, while plasma levels of endogenous testosterone changed little. (j Clin Endocrinol Metab 63: 1361, 1986)
Testosterone propionate-19-d3 administration studies
The study subjects were two normal men, 27 and 24 yr old, weighing 72 and 61 kg, respectively. To determine the secretory dynamics of endogenous testosterone, heparinized blood samples (10 ml) were obtained at 0800; 1100, 1400,1700, and 2000 h for 4 days. The men then were given 25 mg testosterone propionate-19-d3, IM, at 0800 h. Ten-milliliter heparinized blood samples were obtained 5 min before and 3, 6, 9, 12, 24, 27, 30, 33, 36, 48, 54, 60, 72, 78, and 84 h after dosing. Plasma was separated by centrifugation and stored at -20 C until analysis.
Results
Endogenous plasma testosterone profiles
Before studying the disposition of testosterone propionate, we determined the levels of endogenous plasma testosterone for 4 days in the two normal men (Fig. 1). The mean plasma testosterone concentration in subject 1 was 6.6 ng/ml, with a range of 4.0-8.9 ng/ml. Subject 2 had a mean value of 6.9 ng/ml and a range of 4.7-9.3 ng/ml. Testosterone concentrations had a circadian rhythm, with the highest levels between 0800 and 1100 h and the lowest levels between 1700 and 2000 h in both men.
FIG. 1. Plasma testosterone profiles in subjects 1 and 2.
Plasma testosterone propionate-19-d3 and testosterone19-da concentrations
Plasma testosterone propionate-19-d3 levels were maintained at 2-4 ng/ml between 3 and 36 h after IM administration of a single 25-mg dose of testosterone propionate-19-d3 (Fig. 2) and thereafter decreased very slowly. Testosterone-19-d3 was detected in the first blood sample taken 3 h after the injection. The maximum plasma testosterone-19-d3 levels (15.0 ng/ml for subject 1 and 11.5 ng/ml for subject 2) occurred between 24 and 27 h. Thereafter, the decline of testosterone-19-d3 was parallel to that of testosterone propionate-19-d3 in both subjects. The pharmacokinetic parameters characterizing the disposition of testosterone propionate-19-d3 and testosterone-19-d3 are summarized in Table 1.
Effect of testosterone propionate-19-d^ on plasma endogenous testosterone
Endogenous plasma testosterone levels were measured at various times for 84 h after the IM testosterone propionate-19-d3 injection. The results are shown in Fig. 2. Endogenous testosterone levels just before the administration of testosterone prOpionate-19-d3 were 7.2 ng/ml in subject 1 and 7.5 ng/ml in subject 2. After the administration of testosterone propionate-19-d3, endogenous testosterone levels varied between 3.8 and 7.8 ng/ml and 4.4 and 7.5 ng/ml in subjects 1 and 2, respectively.
FlG. 2. Plasma concentrations of testosterone propionate-19-d3 (■ ■), testosterone-19-d3 (O O), and endogenous testosterone (• •) vs. time in subjects 1 and 2. An IM dose of 25 mg testosterone propionate-19-d3 was given to the two normal men at 0800 h
Discussion
The use of GC-MS and stable isotopically labeled drugs as tracers make it possible to provide a precise analytical method for both the parent compound and metabolites with high sensitivity and selectivity (20-22). The application of this method allowed us to follow the plasma levels of testosterone propionate-19-d3 and its active metabolite testosterone-19-d3 for 84 h after the IM administration of testosterone propionate-19-d3.
Intramuscularly administered testosterone propionate-19-d3 was readily detected in the circulation, demonstrating clearly that the testosterone propionate-19-d3 was transferred from the injection site in the muscle to the systemic circulation.
*Nieschlag et al. (8) measured the total plasma exogenous and endogenous testosterone levels by RIA after the IM administration of 25 mg testosterone propionate to normal men. Total plasma testosterone levels were maintained above the physiological levels for 24 h after drug administration. However, it was not possible to determine exactly the contribution of administered testosterone propionate to the total concentration of circulating testosterone. With the aid of the double isotope dilution assay employed in this study, endogenous testosterone and testosterone derived from administered testosterone propionate could be differentiated easily. Conversion of testosterone propionate-19-d3 to testosterone-19-d3 was fast in the systemic circulation, and testosterone propionate-19-d3 injection resulted in exogenous testosterone levels above the normal testosterone level (>4 ng/ml) for 48 h. Moreover, exogenous testosterone continued to contribute to the total plasma levels for up to 84 h.
Attachments
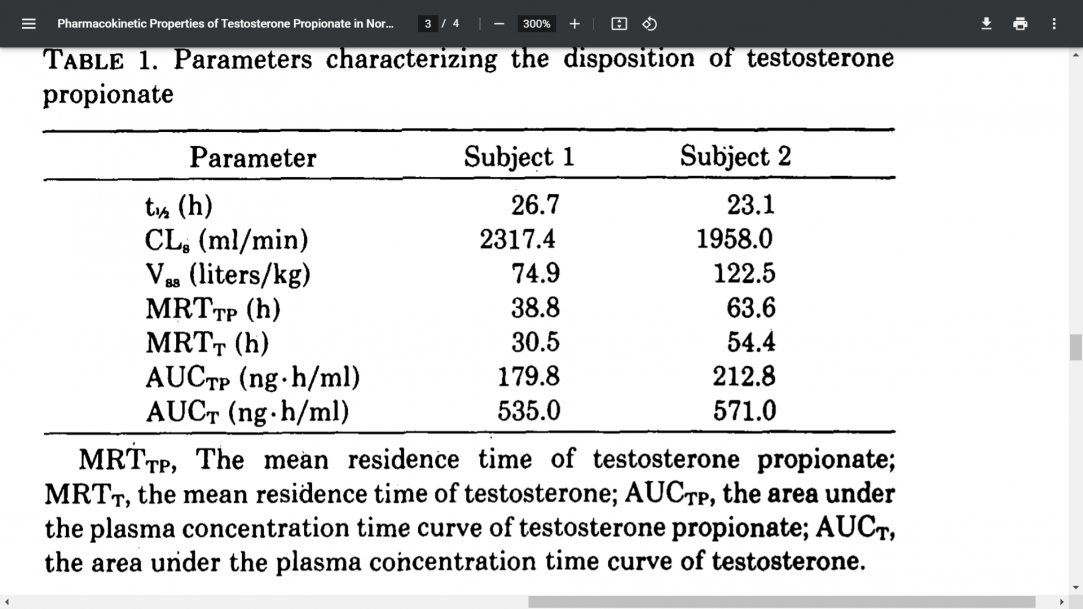
This study has puzzled me in the past. If you superimpose the data to simulate daily injections then you see very subdued daily variation in serum testosterone. I posted one of them here. Thanks to some of your other posts I'm aware that the presence of benzyl alcohol can increase the absorption rate of testosterone esters. In this study: "The (19-2H3)testosterone propionate preparation for i.m. injection was prepared by dissolving 25 mg (19-2H3)testosterone propionate in 1 ml sesame oil containing 20% benzyl benzoate, ...." Do you know if benzyl benzoate has less of an effect on the rate of absorption than benzyl alcohol? The large depot size relative to testosterone content may also help to extend the apparent half-life...
Pharmacokinetic Properties of Testosterone Propionate in Normal Men (1986)
...
madman
Super Moderator
This study has puzzled me in the past. If you superimpose the data to simulate daily injections then you see very subdued daily variation in serum testosterone. I posted one of them here. Thanks to some of your other posts I'm aware that the presence of benzyl alcohol can increase the absorption rate of testosterone esters. In this study: "The (19-2H3)testosterone propionate preparation for i.m. injection was prepared by dissolving 25 mg (19-2H3)testosterone propionate in 1 ml sesame oil containing 20% benzyl benzoate, ...." Do you know if benzyl benzoate has less of an effect on the rate of absorption than benzyl alcohol? The large depot size relative to testosterone content may also help to extend the apparent half-life
Both are solvents and enhance the solubility/reduce the viscosity of the prodrug.
Mind you it would come down to the concentration used.
Most esterified injectable T preparations tend to use BOH as the main excipient.
Some use both although BOH tends to be a higher concentration.
My reply from a previous thread:
Regarding half-lives keep in mind that a majority of studies on the PK/PD of the various T-esters were done using IM (once weekly/fortnightly) injections in a small number of subjects and most of the literature is from decades ago.
There are many other factors that affect the rate at which the testosterone is released from the oily depot at the injection site.
Sub-q vs IM, the volume of injection, injection depth, site of injection, lymphatic flow, the concentration of BOH (benzyl alcohol) are other possible factors that can affect absorption rates of the esterified hormone.
I have stated in the past that BOH apparently causes a large bolus of the prodrug to be released earlier which was discussed in this paper (NEW INSIGHTS INTO DRUG ABSORPTION FROM OIL DEPOTS) that I posted in a thread from 2018
*It is demonstrated in this dissertation that there is a role of the excipient BOH in yielding an initially high absorption.
I know there are even nandrolone studies showing that the addition of BOH (benzyl alcohol) which is commonly used in many injectable preparations has been shown to cause two distinct peaks.....one early and another days later as the BOH apparently causes a large bolus of the prodrug to be released early.
Benzyl alcohol (BOH) is a commonly used excipient in oil depots in concentrations ranging from 1.5-10% v/v and is used as a
*solubility enhancer
*oil viscosity reducer
*local anesthetic
*The absorption of nandrolone is enhanced by the presence of benzyl alcohol. This is most likely an effect of altered OIL VISCOSITY and partition coefficient between the oil and aqueous phase. The absorption rate constant of compounds is found to be related to the logP of the SOLUBILIZED PRODRUG. The absorption rate is however not only determined by the Physico-chemical properties of the formulation but also by the TISSUE PROPERTIES. Here, it is argued that LYMPHATIC FLOW must be considered as a relevant parameter.
NEW INSIGHTS INTO DRUG ABSORPTION FROM OIL DEPOTS
Besides the oil component, an additional excipient in oil depots is benzyl alcohol (BOH) (see Table 1.1). The main function in oil depots is that it enhances the solubility of the processed lipophilic prodrugs (Table 1.3). The second function of BOH is to ease the administration because of its viscosity-reducing effect.
The last function of BOH is that it acts as a local anesthetic. Other frequently used excipients are benzyl benzoate (BBA) and ethanol (EtOH). An overview is given in Table 1.3 below
Table 1.3: An overview of other frequently used excipients in oil depots
Bigben
Member
Prop only dried me out to much. Good it works for you.See my post on page 2. In a nutshell, I had to discontinue my attempt at the blended protocol using Cyp + Prop @ 1.2:1 ratio due to water retention from the cypionate. It's a problem that I've experienced before with larger doses of cypionate.
I am back on Propionate-only at 8mg per day and doing pretty well although I would have preferred the blend. I am going put together some notes in the coming weeks on my experience trying to tame the wild mustang of low dose daily Prop.
ivkonst2017
Active Member
What do you mean dry out? Propionate usually converts more into estrogen in comparison to cypionateProp only dried me out to much. Good it works for you
If you mean increased water retention, I get zero on Propionate whereas I gained 15lbs on cypionate which is not uncommon on this forum. I view that as a major advantage of prop from a health perspective.Prop only dried me out to much. Good it works for you.
Bigben
Member
So 'they' say. I've been doing yet for years. Tried every protocol out there. In my and others I know you use it it does the opposite. Why do you think my friends who compete switch to it end of cycle pre comp. Or any pro for that matter. Certainly not cus it aromatizes more. It's simple. Mix half e half p. Way better than each on their own. Daily works best with slin. Baby dose of .1 ml. Boom ur done. Constant boners. Hardcore workouts. Throw in some HCG and hmg for a few weeks here and there. Never used a adex Asin or Petro since doing this. And I walk around looking jacked more than guys doing gear.What do you mean dry out? Propionate usually converts more into estrogen in comparison to cypionate
ivkonst2017
Active Member
Im a fan of sustanon thats what works best for me and it is the cheaepest one here, also no pharma prop in my countrySo 'they' say. I've been doing yet for years. Tried every protocol out there. In my and others I know you use it it does the opposite. Why do you think my friends who compete switch to it end of cycle pre comp. Or any pro for that matter. Certainly not cus it aromatizes more. It's simple. Mix half e half p. Way better than each on their own. Daily works best with slin. Baby dose of .1 ml. Boom ur done. Constant boners. Hardcore workouts. Throw in some HCG and hmg for a few weeks here and there. Never used a adex Asin or Petro since doing this. And I walk around looking jacked more than guys doing gear.
is that 5mg or each per day or you mean half a ml of e and half a ml of prop mixed and take .1ml a day meaning 12.5mg of e a day and 5mg of prop a daySo 'they' say. I've been doing yet for years. Tried every protocol out there. In my and others I know you use it it does the opposite. Why do you think my friends who compete switch to it end of cycle pre comp. Or any pro for that matter. Certainly not cus it aromatizes more. It's simple. Mix half e half p. Way better than each on their own. Daily works best with slin. Baby dose of .1 ml. Boom ur done. Constant boners. Hardcore workouts. Throw in some HCG and hmg for a few weeks here and there. Never used a adex Asin or Petro since doing this. And I walk around looking jacked more than guys doing gear.
Bigben
Member
Yes mix both equally. Yes that's what it works out to in .1 ml a day which is a baby dose really.is that 5mg or each per day or you mean half a ml of e and half a ml of prop mixed and take .1ml a day meaning 12.5mg of e a day and 5mg of prop a day
Bigben
Member
I actually just switched back to my other routine a few days ago. 10 mg suspension daily. Why? I get more bang for the amount. Here is the calculator to show. You can type in the 12.5 and 5 mg week 1 to 5 then 10 mg suspension week 6 to 10.is that 5mg or each per day or you mean half a ml of e and half a ml of prop mixed and take .1ml a day meaning 12.5mg of e a day and 5mg of prop a day

Steroid Plotter - The Web's #1 Steroid Cycle Planner
SteroidPlotter is the leading steroid cycle planner on the Web. Plot graphs and calculate levels for Anabolic Steroids (Testosterone, Nandrolone and more), TRT & Peptides based on dosage & half-life.
Sponsors










Online statistics
- Members online
- 9
- Guests online
- 9
- Total visitors
- 18
Totals may include hidden visitors.
Latest posts
-
-
-

-

-

-
-
Free Testosterone targets for the best Libido
- Latest: Cyclingislife
-

-
© Copyright 2020 ExcelMale