PAUL-E
Member
They are not my results My IGF-1 is already high on TRT 374 115-307. but I can answer for the test subjectPaul-E
How is your appetite? Have you gained weight? How are you sleeping?
no noticeable appetite change
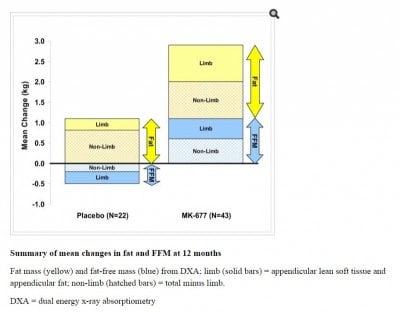
gained some LBM lost some fat
improved sleep less waking moving at night
add
improved skin/hair
improved libido
improved mood
reduced soreness