
@Cataceous - are you still on your GnRH protocol? What have you tweaked about it over time?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Is GnRH suppression hurting us?
- Thread starter Cataceous
- Start date
-
- Tags
- gnrh hpta suppression


Yes, still on the GnRH protocol with 20 mcg 5.25x daily along with TRT and enclomiphene. For the last two months I've taken 5 or 10 mcg kisspeptin-10 along with each GnRH dose. This has correlated with a significant enhancement of nocturnal erections, in a dose-dependent manner.@Cataceous - are you still on your GnRH protocol? What have you tweaked about it over time?
A tip of the hat to @ajax31 for an interesting link involving GnRH and cognition. It appears that a lack of GnRH contributes to cognitive deficits in Down Syndrome.

 futurism.com
futurism.com
See also:

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Other comments related to the work:

Scientists Say New Treatment May Improve Cognition for People With Down Syndrome
According to new research, there may be ways to improve or even reverse disabilities associated with Down syndrome with the use of a new hormone treatment.
futurism.com
In a pilot experiment involving mice with three copies of chromosome 21, a team led by neuroscientist Vincent Prevot of the University of Lille in France found that increasing the levels of GnRH using microRNAs was able to reverse the effects Down syndrome had on the animals' olfactory senses and other cognitive deficits.
Of course, an animal study doesn't prove anything for humans. But a followup experiment involving seven men with Down syndrome who received GnRH from a pump under their skin showed hopeful results as well.
"Six out of seven patients improved their cognitive tests by 20 to 30 percent," Prevot told Scientific American.
"Even more amazing, we saw that functional connectivity was tremendously increased in all seven in cortical areas involved in speech and 3D orientation," Prevot added, noting that the men experienced improvements in verbal comprehension and temporary memory and attention.
See also:
GnRH replacement rescues cognition in Down syndrome - PubMed
At the present time, no viable treatment exists for cognitive and olfactory deficits in Down syndrome (DS). We show in a DS model (Ts65Dn mice) that these progressive nonreproductive neurological symptoms closely parallel a postpubertal decrease in hypothalamic as well as extrahypothalamic...
pubmed.ncbi.nlm.nih.gov
GnRH thus plays a crucial role in olfaction and cognition, and pulsatile GnRH therapy holds promise to improve cognitive deficits in DS.
Other comments related to the work:
GnRH therapy improves cognition in patients with Down syndrome
Gonadotropin-releasing hormone (GnRH) therapy improves cognitive function in Down syndrome (DS) mouse models and male patients with DS, according to a new study. The findings reveal a previously underappreciated role of GnRH – a hormone commonly associated with fertility and reproduction – in...
www.eurekalert.org
Recent research has suggested that olfaction loss and male infertility is also a characteristic of GnRH deficiency, and that GnRH may play a role in higher brain functions, such as cognition.
tropicaldaze1950
Well-Known Member
This might be only tangential or even irrelevant to your post but here it goes. Before going on TRT, I went through a period where I was eating salmon burgers/canned salmon several times a week and taking fish oil, too, all at the recommendation of my then psychiatrist, in the hope of stabilizing my untreatable bipolar illness. Also using several tablespoons of olive oil, daily(cooking & salads). I also had ED for 7 years. Had labs drawn by my endo. TT was 668. FT 110 E2 34. Lipid profile was excellent. This was Kaiser Mid-Atlantic. I was fortunate to get a most basic, though inadequate, hormone panel. My point; no exogenous T to suppress GnRH, LH, FSH. I did have sexual desire, sometimes intense, attributable to elevated mood.I've felt a blunting of emotions during two conditions: with a combination of high testosterone and high estradiol; and with very low estradiol. With normal testosterone and high estradiol I felt an amplification of emotions.
It would be great if GnRH were this "missing piece" for libido, but when is anything TRT-related ever that simple?
The findings of the research you site are interesting. And as you said, "When is anything TRT-related ever that simple?"
Here's a study looking at an apparent protective effect of GnRH in rats, which acts via enhancing estradiol in the hippocampus. If I'm interpreting this correctly, they're saying that the effect is not via regulation of estradiol synthesis, because "Letrozole did not reverse GnRH modulatory effects on hippocampal E2 levels and neuroprotection."
pubmed.ncbi.nlm.nih.gov
Introduction: The 17β-estradiol (E2) enhances hippocampal dendritic spine synapses, facilitates learning processes, and exerts neuroprotection. Brain estrogen decline has been reported in Alzheimer's disease. The role of GnRH in modulating steroid biosynthesis convinced us to examine whether hippocampal GnRH administration could enhance the local E2 levels and overcome the development of cognition decline in amyloid β (Aβ) neurotoxicity. To explore if GnRH acts through regulating E2 synthesis, letrozole, an aromatase inhibitor, has been applied in combination with GnRH.
Methods: Female rats received an intracerebroventricular injection of Aβ. The GnRH and, or letrozole were injected into the CA1 for 14 consecutive days. Working memory, novel object recognition memory, and anxiety-like behavior were evaluated. Serum and hippocampal E2 levels were measured. Hippocampal mRNA expression of GnRH (GnRH-R) and E2 (ERα and ERβ) receptors was assessed. GnRH effect on the excitability of pyramidal cells was studied by in vivo single-unit recording.
Results: GnRH increased hippocampal E2 levels, evoked an increase in the spontaneous firing of pyramidal neurons, and caused mRNA overexpression of hippocampal GnRH receptors. GnRH prevented the adverse effects of Aβ on working memory, NOR index, and anxiogenic behavior. Letrozole did not reverse GnRH modulatory effects on hippocampal E2 levels and neuroprotection.
Conclusion: GnRH prevented the Aβ-induced memory deficit, which may be mediated through hippocampal E2 levels enhancement. The electrophysiological analysis revealed the enhanced neuronal excitability in the CA1 region. All these data suggest that GnRH might be a promising candidate that reduces anxiety and improves memory indices in the context of Aβ neurotoxicity.
GnRH protective effects against amyloid β-induced cognitive decline: A potential role of the 17β-estradiol - PubMed
GnRH prevented the Aβ-induced memory deficit, which may be mediated through hippocampal E2 levels enhancement. The electrophysiological analysis revealed the enhanced neuronal excitability in the CA1 region. All these data suggest that GnRH might be a promising candidate that reduces anxiety and...
pubmed.ncbi.nlm.nih.gov
tropicaldaze1950
Well-Known Member
You're addressing the issues I've been dealing with for years while on TRT, though what I experience is being emotionally flat, near constant sadness and cognitive blunting. Higher dosing of testosterone makes it feel like my brain is separated from my body; I feel less connected to myself and to my surroundings.As you’ve probably experienced at some point, there’s definitely something that causes blunted emotions, especially with higher doses. It’s almost like things that should make a person sad simply don’t have an effect. I think it could possibly factor into libido as well because there’s such a vast amount of chemicals and neurotransmitters that play a part in arousal. Perhaps this missing piece could actually play a bigger role in libido than testosterone, estrogen or dopamine.
Last edited:
Most of it I’ve dealt with by simply going lower with the dose. I only use 60mg per week and all aspects are much better.You're addressing the issues I've been dealing with for years while on TRT!
tropicaldaze1950
Well-Known Member
Lowering my dose is something I was pondering. How often do you inject?Most of it I’ve dealt with by simply going lower with the dose. I only use 60mg per week and all aspects are much better.
Once a week. I’ve tried splitting the dose but have to do 72-80mg to feel the same.Lowering my dose is something I was pondering. How often do you inject?
tropicaldaze1950
Well-Known Member
Thanks.Once a week. I’ve tried splitting the dose but have to do 72-80mg to feel the same.
tropicaldaze1950
Well-Known Member
This is a most informative thread! Its sent me off to do research on PubMed. Question: Testosterone and E2 suppress GnRH; not for every man, but for a % of men. Why not, without testosterone, microdose or ultramicrodose anastrazole, whether daily or 2 or 3 times a week? 1/10th of a milligram or even less? I know my thinking is mechanistic. I've read that E2 is higher in the hypothalamus and pituitary than peripherally. Whether in theory or in fact, lowering E2 in the brain, either should or does, increase T/free T with a possible improvement in erectile function. I've said that I'm at the point of giving up on testosterone, but the information and discussion, here, has given me another perspective.
FunkOdyssey
Seeker of Wisdom
I suspect you get similar benefits to this local production by simply having a lot of estradiol floating around the body and letting it diffuse across the blood brain barrier. I also don't think high levels of GnRH are as helpful for dementia protection in humans as this study suggests. Why?Conclusion: GnRH prevented the Aβ-induced memory deficit, which may be mediated through hippocampal E2 levels enhancement.
Well, who has the highest GnRH levels? Menopausal women. Who has the highest rates of dementia? Menopausal women. How do you reduce their risk of dementia? You give them estradiol:

Systematic review and meta-analysis of the effects of menopause hormone therapy on risk of Alzheimer’s disease and dementia
IntroductionDespite a large preclinical literature demonstrating neuroprotective effects of estrogen, use of menopausal hormone therapy (HT) for Alzheimer’s disease (AD) risk reduction has been controversial. Herein, we conducted a systematic review and meta-analysis of HT effects on AD and...
In a significant majority on TRT there is nearly complete suppression. This is evidenced by low levels of LH and FSH.... Question: Testosterone and E2 suppress GnRH; not for every man, but for a % of men.
AI monotherapy has been proposed as a way to increase endogenous testosterone, and there's at least one study on anastrozole claiming success. However, the long-term effects are uncertain.Why not, without testosterone, microdose or ultramicrodose anastrazole, whether daily or 2 or 3 times a week? ...
These data demonstrate that aromatase inhibition increases serum bioavailable and total testosterone levels to the youthful normal range in older men with mild hypogonadism. Serum estradiol levels decrease modestly but remain within the normal male range. The physiological consequences of these changes remain to be determined.
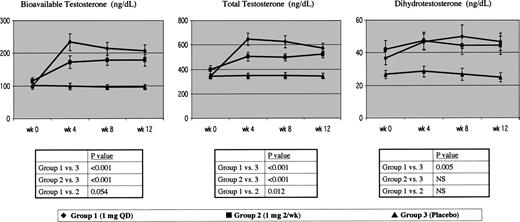
Effects of Aromatase Inhibition in Elderly Men with Low or Borderline-Low Serum Testosterone Levels
Abstract. As men age, serum testosterone levels decrease, a factor that may contribute to some aspects of age-related physiological deterioration. Although
 academic.oup.com
academic.oup.com
I suspect you get similar benefits to this local production by simply having a lot of estradiol floating around the body and letting it diffuse across the blood brain barrier. I also don't think high levels of GnRH are as helpful for dementia protection in humans as this study suggests. Why?
Well, who has the highest GnRH levels? Menopausal women. Who has the highest rates of dementia? Menopausal women. How do you reduce their risk of dementia? You give them estradiol:
Systematic review and meta-analysis of the effects of menopause hormone therapy on risk of Alzheimer’s disease and dementia
IntroductionDespite a large preclinical literature demonstrating neuroprotective effects of estrogen, use of menopausal hormone therapy (HT) for Alzheimer’s disease (AD) risk reduction has been controversial. Herein, we conducted a systematic review and meta-analysis of HT effects on AD and...www.frontiersin.org
LH is probably involved.
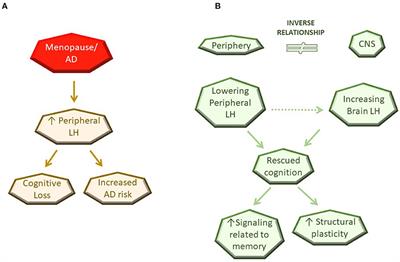
Luteinizing Hormone Involvement in Aging Female Cognition: Not All Is Estrogen Loss
Pervasive age-related dysfunction in hypothalamic-pituitary-gonadal (HPG) axis is associated with cognitive impairments in aging as well as pathogenesis of age-related neurodegenerative diseases such as the Alzheimer's disease (AD). As a major regulator of the HPG axis, the steroid hormone...
Together, these data suggest that while estrogen is relevant and important for CNS function and structure during the reproductive periods, aspects beyond estrogen loss contribute to age-related menopausal dysfunction.
...
In fact, increased levels of peripheral LH in AD patients is associated with exacerbated pathology and cognitive deficits (50–52). Additionally, increased LH is correlated with increased plasma Aβ1−40 and Aβ1−42 levels in subjective memory complainers, suggesting LH may play a progressive role in early preclinical stages (51).
tropicaldaze1950
Well-Known Member
Before starting on testosterone in 2013, I did have inconsistent, but strong erections. My total, pre TRT, was 360 ng/dL. There were significant marital problems which shutdown desire for my wife, as well as the emotional toll of no longer being able to work due to bipolar illness. Now I'm my wife's caregiver.
I did my due diligence on testosterone therapy. It wasn't just suddenly deciding. I either read or was on multiple forums. Maybe, for me, I'm considering that testosterone is the source of problems, rather than benefits. Still trying to figure it out.


Sponsors









Online statistics
- Members online
- 6
- Guests online
- 4
- Total visitors
- 10
Totals may include hidden visitors.

© Copyright 2020 ExcelMale