
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.


Curious - were you worked up and dx'd as hypopit by an endo? Did the MRI reveal any pituitary anomalies (i.e. empty sella)? I'm assuming your GH stim test showed AGHD?IF it were me, I would want to know if your Secondary Hypogonadism, or primary Hypogonadism. I would also then want more evaluation on that cortisol, by testing am cortisol and acth serum. I would also want to know DHEA-s levels, IgF-1 . IF your secondary which is what I was, I also had low saliva cortisol, I ended up getting a Itt stim and glucagon stim for Growth hormone deficiency and sai (secondary adrenal insuficiency) I am Pan Hypo Pituitary as it turns out and I replace all those hormones. You will also need a MRI of the pituitary too
Curious - were you worked up and dx'd as hypopit by an endo? Did the MRI reveal any pituitary anomalies (i.e. empty sella)? I'm assuming your GH stim test showed AGHD?
I was worked up and diagnosed by an endo. The ITT stim and glucagon stim is what I had and I stimmed to .5 with 5 or less passing so it was very low. However, parts of my treatment were not working such as thyroid. I have a diodinase gene defect and I had super high reverse t3 that he would not test or do anything and my free t3 was super low. Then I ended up going to a functional medicine doctor and she has me on mostly t3 and a little t4. MRI did not reveal anything. I have iron overload that causes that and had it many years. I also have a traumatic brain injury when I was 15 yrs old which makes sense as that is when the weight gain and severe fatigue started. I cannot tell you how many times people have had repeated MRIs and then get another one that shows all kinds of things.
That is definitely suspicious. If it were me I would be getting a Insulin tolerance test or a metyrapone stim test , that I will tell you.ACTH was ran by a doctor years ago. My value was 12 on a range from 7-69, and this was drawn late-at 3pm.
Blood cortisol was 12, range of 2-23, drawn at the same time.
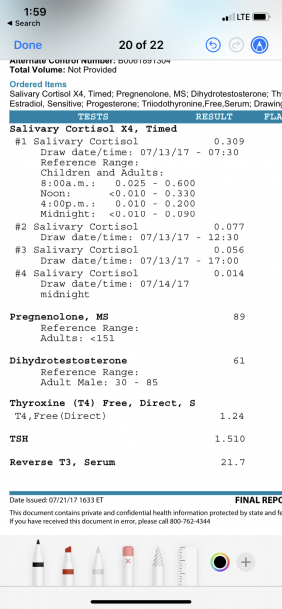
Saliva cortisol was done once, years after the above test. My 8am value was .300, upper range was .600, and by noon the number dropped ridiculously low- I’ll try to find the Labcorp results.
If iron saturation was high I wonder what ferritin was ? Iron saturation should ideally be 25 t 35 % damage occurs above 45%. That sounds like iron overload to me.FH and LSH are around 5-7. I have new labs coming soon.
SHBG was only 37 my first time testing, but has always been in the 50s ever since. On a vegan diet shbg was in the 80s.
I am retrying a low iron diet. I was feeling good on low iron, no red meat, and doing this “Root Cause” protocol that focuses on reducing unbound iron. I slipped up on cereal fortified with iron, or my body went back to this symptomatic state.
-I have had 2 iron tests, one had a high saturation, next one was in range.
I was worked up and diagnosed by an endo. The ITT stim and glucagon stim is what I had and I stimmed to .5 with 5 or less passing so it was very low. However, parts of my treatment were not working such as thyroid. I have a diodinase gene defect and I had super high reverse t3 that he would not test or do anything and my free t3 was super low. Then I ended up going to a functional medicine doctor and she has me on mostly t3 and a little t4. MRI did not reveal anything. I have iron overload that causes that and had it many years. I also have a traumatic brain injury when I was 15 yrs old which makes sense as that is when the weight gain and severe fatigue started. I cannot tell you how many times people have had repeated MRIs and then get another one that shows all kinds of things.
How did you ascertain you had a deiodinase SNP?
Do you know which type(s) (I, II, III)?
There are several SNPs for this. Approx. two out of ten people have these SNPs. But to what effect they actually manifest clinically is unknown - and unfortunatley disregarded as clinically insignificant by 99% of all endos. We can speculate that some of the ones in which you don't carry the polymorphism may neutralize the ones you do, hence, a wash, or perhaps slightly impaired fuction of this enzymatic conversion of T4 to T3. Very complex science where endos know very little which is why they assume everyone converts to some degree, prescribe the cookie-cutter T4 meds, and call it a day. Pathetic.
On a side note, have you looked into peptides for TBI?
LH and FSH are always normal. SHBG is high, so testosterone is normal on lab tests. DHEA is low, IGF is normal(180)
Dr Saya analyzed my cortisol
-Said morning was half of what it should be
-Said by noon it dropped really low
-Said evening was almost zero
No medicine besides DHEA/pregnenalone pills
I have never heard anything besides ACTH stimulation. It seems impossible to even find an endocrinologist that has any experience or knowledge to do what you recommended. And I’ve seen 4 of them.
Perhaps, 10mg Hydrocortisone upon waking.
How did you ascertain you had a deiodinase SNP?
Do you know which type(s) (I, II, III)?
There are several SNPs for this. Approx. two out of ten people have these SNPs. But to what effect they actually manifest clinically is unknown - and unfortunatley disregarded as clinically insignificant by 99% of all endos. We can speculate that some of the ones in which you don't carry the polymorphism may neutralize the ones you do, hence, a wash, or perhaps slightly impaired fuction of this enzymatic conversion of T4 to T3. Very complex science where endos know very little which is why they assume everyone converts to some degree, prescribe the cookie-cutter T4 meds, and call it a day. Pathetic.
On a side note, have you looked into peptides for TBI?
Genetic testing different ones came up some time when I have time I will look for that. I did that testing for the doctor but it didnt matter t4 t3 / t4 combo ndt thyroid compounded it didnt matter i felt horrible on all of those for 20yrs All I would end up with is super high reverse t3 way over the range and low t3 levels either below the range or barely in range. As a matter of fact the last endo i got up to 4 grains after about a year My free t3 was barely in range and he looked at me and his answer to my issue was that I wasnt taking it. wth has Anything including inflammation can cause conversion issues with elevated reverse t3. There is also growth hormone deficiency testosterone deficiency low iron and many others. I suspect hemochromatosis might be another reason why mine is thet way not sure snd honestly I dont care lol
Last edited:
I have not looked into peptides but interesting to look into Thank you If you have info on peptides or any other therapy post that up I am all about thatHow did you ascertain you had a deiodinase SNP?
Do you know which type(s) (I, II, III)?
There are several SNPs for this. Approx. two out of ten people have these SNPs. But to what effect they actually manifest clinically is unknown - and unfortunatley disregarded as clinically insignificant by 99% of all endos. We can speculate that some of the ones in which you don't carry the polymorphism may neutralize the ones you do, hence, a wash, or perhaps slightly impaired fuction of this enzymatic conversion of T4 to T3. Very complex science where endos know very little which is why they assume everyone converts to some degree, prescribe the cookie-cutter T4 meds, and call it a day. Pathetic.
On a side note, have you looked into peptides for TBI?
I have dio2 rs225014 c/c dio1 rs2235544 a/c dio1 rs11206244 c/tHow did you ascertain you had a deiodinase SNP?
Do you know which type(s) (I, II, III)?
There are several SNPs for this. Approx. two out of ten people have these SNPs. But to what effect they actually manifest clinically is unknown - and unfortunatley disregarded as clinically insignificant by 99% of all endos. We can speculate that some of the ones in which you don't carry the polymorphism may neutralize the ones you do, hence, a wash, or perhaps slightly impaired fuction of this enzymatic conversion of T4 to T3. Very complex science where endos know very little which is why they assume everyone converts to some degree, prescribe the cookie-cutter T4 meds, and call it a day. Pathetic.
On a side note, have you looked into peptides for TBI?
Honestly, there is nothing wrong with taking more t3, it doesn't have to convert, gets right in there by bypassing all of that. Most people take 50mcg t4 or less and the rest t3 and they are way better by doing that
Stress is a huge reason why RT3 goes up. HC can help. Iodoral (Iodine), Selenium can also help conversion.
No iodine for this guy, really increased tpo antibodies. Selenium actually got elevated so I stopped that selenium rbc tested. hc, yes I take that I am pan hypo pit. along with gh, testosterone, thyroid, fludro,
Perhaps, 10mg Hydrocortisone upon waking.
Everyday? How many days can I stay on it before dependence starts?
I tried methylprednisone but just made me feel a little worse.
If iron saturation was high I wonder what ferritin was ? Iron saturation should ideally be 25 t 35 % damage occurs above 45%. That sounds like iron overload to me.
Yes, iron overload for sure
Everyday? How many days can I stay on it before dependence starts?
I tried methylprednisone but just made me feel a little worse.
It doesn't create dependence. You can go up to about 25mg or a little more per day (spread out). No more than 10mg at a time. Typically start with 10mg upon waking. If needed 5mg more 5 hours later. When I was at my worse, I needed 25mg. As I got better, I weaned down to 10mg at waking. I may be able to when down to 5mg and hopefully off of it. It truly saved me.
You have iron overload. (hemochromatosis. They would probably call that iron avidity since your ferritin does not quite qualify for what most people would have for iron overload. The ferritin would be above 300. non the less That is way to high pretty common finding for hemochromatosis patients in the early stages Not sure how old you are but that saturation is high. Have you donated blood before?
It doesn't create dependence. You can go up to about 25mg or a little more per day (spread out). No more than 10mg at a time. Typically start with 10mg upon waking. If needed 5mg more 5 hours later. When I was at my worse, I needed 25mg. As I got better, I weaned down to 10mg at waking. I may be able to when down to 5mg and hopefully off of it. It truly saved me.
You should never just take hc, one should fine out if they are Secondary adrenal insufficiency. They need a am cortisol and acth serum tested then a Insulin tolerance test or Metyrapone stim test done to see. Also, test for growth hormone deficiency
You should never just take hc, one should fine out if they are Secondary adrenal insufficiency. They need a am cortisol and acth serum tested then a Insulin tolerance test or Metyrapone stim test done to see. Also, test for growth hormone deficiency
I dont agree nor do many physicians. Symptoms alone can tell you if you are having HPA issues
I dont agree nor do many physicians. Symptoms alone can tell you if you are having HPA issues
Well, then you will never know what the actual issue is. If the person has pituitary issues then they need a full workup to see what other hormones they are low in. Just giving hc, that is a very incomplete treatment, what about desmopressin, what about fludrocortisone, what about growth hormone? Very incomplete assessment
That was a few years ago, must have been 25 or so during the test. Have only donated blood once.You have iron overload. (hemochromatosis. They would probably call that iron avidity since your ferritin does not quite qualify for what most people would have for iron overload. The ferritin would be above 300. non the less That is way to high pretty common finding for hemochromatosis patients in the early stages Not sure how old you are but that saturation is high. Have you donated blood before?
I wonder if the hemochromatosis is why I have testicle size fluctuations. I avoided all meat but eggs, and all iron fortified snacks, and testicles got larger/less symptoms/consistent morning wood.
I started eating a box of cereal and symptoms returned.


Sponsors









Online statistics
- Members online
- 4
- Guests online
- 6
- Total visitors
- 10
Totals may include hidden visitors.
Latest posts
-

-
-
-
-

-
Convenient Blood Work Near Me: Locate Lab Test Locations
- Latest: Nelson Vergel
-
-
-

-

© Copyright 2020 ExcelMale