

Nelson Vergel
Founder, ExcelMale.com

Testosterone Is Associated With Reduced All-Cause Mortality and Higher Dihydrotestosterone With Reduced Ischemic Heart Disease Mortality, While Estradiol Levels Do Not Predict Mortality -
In Older Men an Optimal Plasma Testosterone Is Associated With Reduced All-Cause Mortality and Higher Dihydrotestosterone With Reduced Ischemic Heart Disease Mortality, While Estradiol Levels Do Not Predict Mortality
Context:. Testosterone (T) levels decline with age and lower T has been associated with increased mortality in aging men. However, the associations of its
 academic.oup.com
academic.oup.com
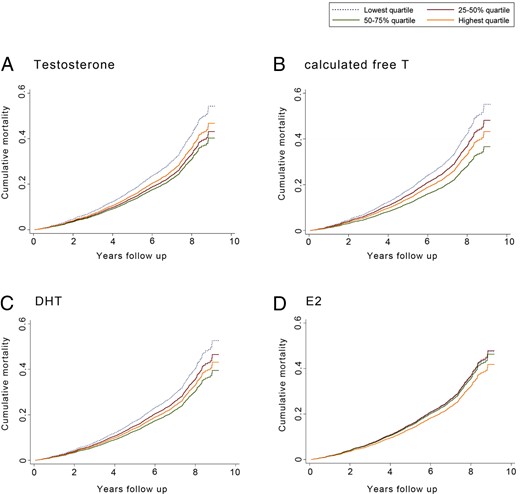
In older men, having total T levels in the middle two quartiles at baseline predicted reduced incidence of death from any cause, as did having calculated free T or DHT levels in the third quartile. These associations could not be explained by age, overweight, or other risk factors, which were adjusted for systematically in the analyses. A higher DHT level was associated with reduced IHD mortality, but E2 was not associated with either mortality outcome.
In previous epidemiological studies generally using immunoassays, lower levels of total or free T have been associated with increased mortality without delineating a U-shaped association (7). For example, a case-control study of men aged 42 to 78 years with 825 deaths and 1489 survivors found reduced all-cause mortality in the third and fourth quartiles of total T (31). In a longitudinal study of 794 men aged 50 to 91 years of whom 538 died during 11.8 years of follow-up, total T in the lowest quartile was associated with increased mortality, with a threshold effect (32). A longitudinal analysis of 1114 younger men aged over 20 years with 206 deaths concluded that lower free T (difference between 90th vs 10th percentile) was associated with all-cause mortality between baseline and 9 years of follow-up (33). There are limited mortality data from studies using mass spectrometry assays for T. In the Swedish Osteoporotic Fractures in Men (MrOS) study of 3104 men aged 69 to 80 years, 383 died during 4.5 years of follow-up. Men with total T in Q2 to Q4 (measured by gas chromatography-mass spectrometry) had lower mortality than those with total T in Q1, with a linear trend (21). Our results challenge the concept that lower T is associated with increased mortality in a linear fashion. Instead, an optimal range of circulating total T corresponding to a range of 9.8 to 15.8 nmol/L (282-455 ng/dL) exists for older men, which predicts survival independent of other risk factors.
Our results differ from those of the Massachusetts Male Aging Study (MMAS) of 1686 men aged 40 to 70 years, in which 395 deaths (101 of IHD) occurred during 15.3 years of follow-up (18). In the MMAS, which used immunoassays for T and DHT and an inaccurate formula to calculate free T, neither T nor DHT was associated with all-cause mortality. Calculated free T was positively associated with deaths of IHD. However, the inverse association of DHT with deaths of IHD was not robust to model selection (18). Our results from a larger cohort of older men using LC-MS/MS for assays of T and DHT indicate that total and accurately calculated free T and DHT had comparable and consistent associations with all-cause mortality. Importantly, in our study, a plasma DHT above the median value (above 1.34 nmol/L [39 ng/dL]) was unequivocally associated with lower IHD mortality risk. Of note, higher plasma DHT was associated with lower all-cause and lower IHD mortality independent of SHBG levels.
There are several factors that might explain the contrast between our results and those of previous studies. The HIMS cohort comprises men aged 70 years and older, whereas other studies have included middle-aged (18, 31, 32) or even younger men (33). It is possible that the biological associations of T and DHT with outcomes such as all-cause or IHD mortality might be accentuated across the transition from middle to older age. In addition, the power of Cox regression models is influenced by the number of outcome events, and we observed 974 deaths (325 of IHD) in our cohort. Therefore, we would expect to define associations with these outcomes more robustly than studies with lower numbers of outcome events. Finally, greater precision from the assay of T and DHT by LC-MS/MS and use of an accurate empirical formula to calculate free T might have improved our ability to characterize their associations with all-cause and IHD mortality in older men.
Previous studies reported that higher E2 levels (measured by immunoassay) were associated with progression of carotid intima-media thickness and with incident stroke (19, 20). The MrOS study in Sweden reported that free E2 (calculated from total E2 measured by RIA using an unvalidated formula) was positively associated with peripheral arterial disease (34). In contrast, the subsequent analysis from the MrOS study found that men with low total E2 (measured by gas chromatography-mass spectrometry) had higher mortality, with the highest mortality rate seen in men with both total T and E2 in the lowest quartile of values (21). However, multivariable adjustment was limited to age, MrOS site, BMI, physical activity, and current smoking. Our results in a larger cohort of older men with more outcome events and comprehensive adjustment for potential confounders indicate that E2 is not associated with all-cause or IHD mortality. This is consistent with previous reports in which plasma E2 was not associated with prevalent CVD or intermittent claudication (28, 35) and with a recent meta-analysis that failed to establish any association of E2 with CVD-related outcomes (36). Therefore, the effects of E2 on the vasculature may be more limited than those in other tissues such as bone (16, 17).
Last edited:












