
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Switching From Cream to Injectable T (subQ)
- Thread starter bkb33
- Start date


madman
Super Moderator
My latest bloodwork results (after switching to injections and adding Danazol 6 weeks ago) are here, and they are – I believe – promising!
My Free T:Total T % is now 1.88%, a marked improvement from the previous 0.77%. That said, the numbers are quite high – but pushing them even higher may, I think, be necessary for me to continue improving. Not sure if I should be worried, though, about how high they’re getting. Free T is more than 3X over the top of the range. Is this sustainable? Is it dangerous long-term? I don't know, given that SHBG is still very high (but much more reasonable now).
My SHBG has dropped from 114 to 72, so the Danazol appears to be working! I’m really encouraged to see this. At the start of this journey, my SHBG was nearly 200.
Of note: Estradiol has gone up to 91. It was 50 before. This seems strange; I guess it happened because T went up so much? I am not on an AI.
I don’t know how to interpret the over-range DHT and Reverse T3 – any cause for concern there? Any other thoughts on these numbers?
Thanks, fellas!


the numbers are quite high – but pushing them even higher may, I think, be necessary for me to continue improving.
Are you kidding me here!
More like absurdly high and no way no how would you need to push your TT/FT levels any higher..... let alone run the TT/FT levels you are hitting and yes even with an SHBG of 72.
You are hitting 2000+ TT levels.....almost close to 3000 ng/dL.....these are levels one would attain on a low dose T cycle!
As I have stated many times before and I will say it again you are using the wrong testing method (direct immunoassay) for testing your FT.
Current problems with accurate free testosterone determination
Current methods for measuring free testosterone (fT) are technically challenging and not accurate. The widely used direct immunoassay and tracer analog techniques for measuring fT have been shown to be inaccurate. Equilibrium dialysis, the reference method against which other methods are compared, is labor-intensive and cumbersome, and therefore has had limited clinical adoption. As an alternative, free testosterone can be computed from the total testosterone, SHBG, and albumin concentrations. Recently, Endocrine Society’s Expert Panel acknowledged the experimental problems in fT measurements and concluded that "...the calculation of free testosterone is the most useful estimate of free testosterone in plasma..." However, we have demonstrated that even the calculated fT values derived from the prevailing equations, based on linear law-of-mass action models or empiric equations, differ systematically from free testosterone measured by equilibrium dialysis by as much as 40%.
Why TruT™?
The only FDA-registered free testosterone calculator
- Improved biophysical characterizations have suggested the importance of models that consider allosteric coupling of testosterone with dimeric SHBG. This model, as implemented by TruT™ provides the most accurate estimates for free testosterone.
- Commonly available free testosterone calculators (issam.ch, nebido.com, pctag.uk) use models of testosterone:SHBG binding (proposed by Vermeulen et al. and Sodergard et. al) which were developed before the crystal structure for SHBG:T complexes were available. These models assume that the two SHBG monomers behave identically in binding testosterone. Detailed experimental data show that the "simplified linear model is erroneous." References.
- The Endocrine Society has issued position statements which highlights the laboratory- and operator-dependent variability inherent in direct free testosterone measurements. For this reason they advocate for indirect "calculator" based methods References.
- The TruT™ calculator provides the ideal solution by using measurements of total testosterone, SHBG, and albumin to calculate free testosterone while taking into account the complex, non-linear allostery in SHBG's association with testosterone. TruT™ is the only calculator available that uses this more complex formulation. References
Forget relying on the older calculated methods let alone direct immunoassay and tracer analog techniques.....either pay to have the gold standard equilibrium dialysis or ultrafiltration or better yet do not spend the money and simply use the newer calculated method TruT Free Testosterone Calculator by FPT
People tend to go on and on and on about high SHBG resulting in low FT.....sure when TT levels are sub-par or low but when TT levels are high enough even with a higher SHBG one can still have healthy FT levels.
Even with an SHBG of 70,80,90,100 as long as TT is high enough one can have a healthy FT......but even then TT will not need to be as high as we used to think due to the complex, non-linear allostery in SHBG's association with testosterone.
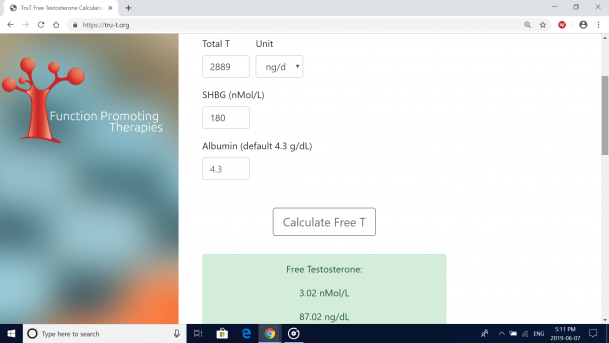
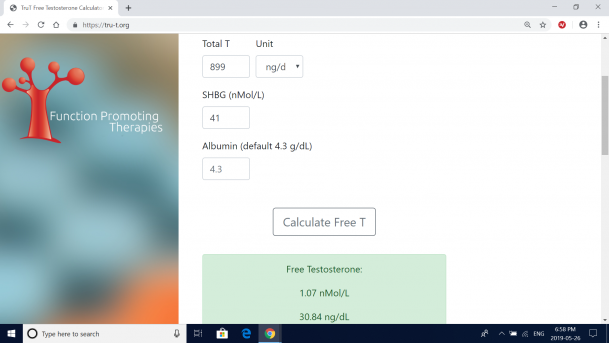
In your case although most would consider an SHBG of 72 nmol/L high seeing as your TT (trough) is absurdly high at 2889 ng/dL than your FT is 103.27 ng/dL (way too f***ing high) above the reference range of 16-31 ng/dL and keep in mind this is using the newer calculated method TruT™ which provides the most accurate estimates for free testosterone.
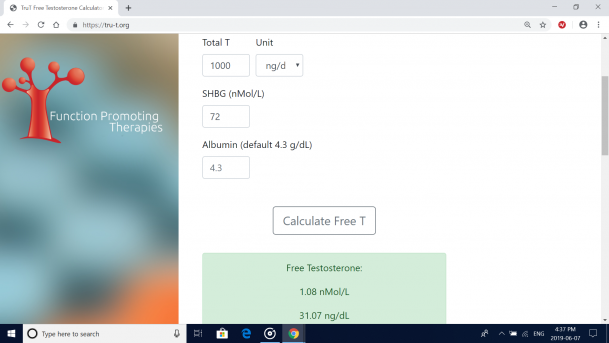
If anything with an SHBG of 72 nmol/L you could get away with running a TT of 1000 ng/dL and your FT would be 31.07 ng/dL (top end of the reference range 16-31 ng/dL)
Most men do well with their FT in the 20-30 ng/dL range and others may need to venture into the 30-50 ng/dL range to see benefits.....but even than many would not need to run FT levels that high let alone be able to tolerate such high levels.
Sure everyone is different and you have to find a level that is best for you within reason and as long as blood markers are in a healthy range and any potential side effects are avoided/minimized.
Overall health is key!
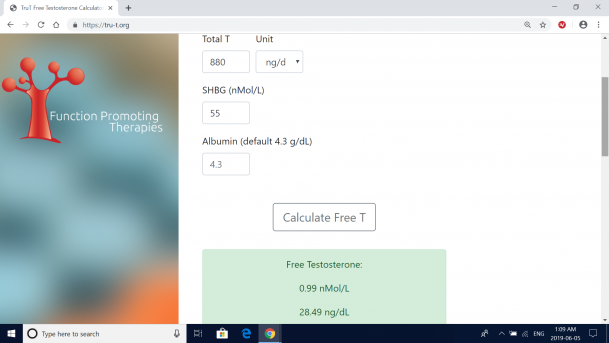
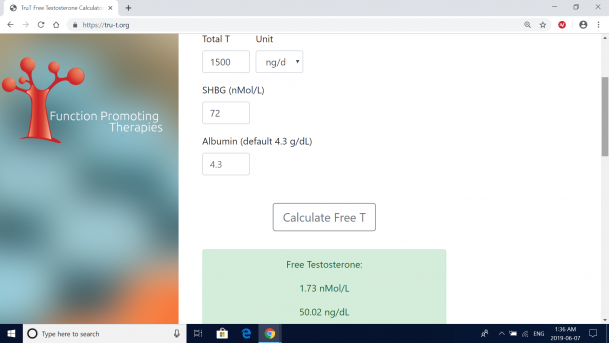
Now to put this in better perspective with an SHBG of 72 nmol/L you would only need to run a TT of 1500 ng/dL which would put your FT levels at a whopping 50.02 ng/dL (well over the top end of the reference range 16-31 ng/dL.
You are using Danazol to lower your SHBG so you should be able to use less T in order to achieve a healthy FT level.....we are not simply trying to hammer down your high SHBG with absurdly high androgen levels!
No way even with your SHBG levels does one need to be running an absurdly high TT of 2889 ng/dL.
You need to rethink this protocol through deeply!
Last edited:
$20Sadly, I didn't have that tested for the 6-week labs. I will have it done next time (in 6 weeks). Wish I had that info!
You need to rethink this protocol through deeply!
I really appreciate the thoroughness of your perspective, and I am indeed rethinking my approach. The reason I mentioned pushing the dose is that my libido is still nowhere in sight -- I have a moderate desire to have sex maybe once every two weeks. Needless to say, this isn't great for my marriage...but perhaps it's an issue I'll have to deal with for the rest of my life, regardless of my T level.
I also, for some reason, would simply feel better about using T monotherapy in the long-term than T + Danazol -- but maybe that belief is unfounded, and I should also plan to stick with Danazol for years to come. It just seems like a less-tested methodology, and also comes with the annoyance of ordering a second (expensive) medication. I think honing in my dose of T alone (plus HCG, which I am taking for fertility) would be ideal.
What do you think would be the best next step, as far as modifying my protocol? I was thinking that perhaps it would be dropping to ~150/week (injecting 75 IU 2X/week). Would you keep Danazol dosage the same (25 mg EOD)?
Last edited:
[QUOTE="madman, Im confused right now, from what i've been reading the last few months is that high SHBG is a problem and goes hand in hand with low FT, the reason that men with elevated shbg have high T is that the testicels keep trying to make up for the lack of available T? Is this completly wrong or? Me 118 SHBG. And walking around with severe complaints that all fall in line with low T.
Im confused right now, from what i've been reading the last few months is that high SHBG is a problem and goes hand in hand with low FT, the reason that men with elevated shbg have high T is that the testicels keep trying to make up for the lack of available T? Is this completly wrong or? Me 118 SHBG. And walking around with severe complaints that all fall in line with low T.
That is correct. Having SHBG too high or too low is a problem. And indeed, high SHBG is correlated with lower FT. However, though my SHBG (72) is still quite high, it is not nearly what it once was (180+). Further, my Free T has climbed quite high, high enough to overcome the still-high SHBG, as a result of the introduction of T-cypionate being injected.
If you have an SHBG of 118 and are not taking exogenous T into your system, it is quite likely -- perhaps all but certain -- that you do have low Free T.
@madman
My follow-up with my provider today went well. We are going to lower my dosage from 200mg/week to 180/week; switch from 2X/week injections to 3X/week; and aim to lower estrogen by increasing Danazol dosage. Further, I need to continue monitoring T3 and increase my caloric consumption.
He wasn’t overly concerned about the high numbers. Right now, my Free T is 54.3 (using the decimal-point conversion system), and we are hoping to see it around 40 next time around. We are also hoping to see SHBG go down more and E go down.
Our meeting largely focused on estrogen. He says our goal is to get the E number to be lower than the SHBG number.
He gave me the flexibility to decide how much to increase my Danazol dosage and was happy to go up to 25 mg ED (previously: 25 mg EOD). I’m hoping for some insight here. I was thinking I would do 25 mg 5X/week. My goal is to get SHBG under 50 (was 72 on these recent bloods after starting at 180 at the beginning of HOT). How much would you increase it? Would you go up to 25 mg ED? I do not want to employ an AI, though I do have some on hand if needed.
It seems Danazol will intermittently be a part of my protocol for the foreseeable future. Once we get SHBG sufficiently low — which will allow me to have a more moderate T level — we will lay off the Danazol for a while, then reintroduce it if SHBG increases too much. This cycling system will be in place to reduce the risk of liver toxicity. That liver toxicity possibility is why I'm not ruling out an AI entirely. It may need to come into play at some point.
We also talked a lot about my high Reverse T3. He believes this is a result eating too few calories — something he sees a lot in bodybuilders who do caloric restriction. He believes I should be eating a lot more (currently: all the way down to 1800 cals, as I have been cutting for 2 months). My T3 is now 9% of my Reverse T3, and our goal is for it to be 20% or more. But raising thyroid hormones can also raise SHBG, so we are going to leave this alone for now and just roll with the other changes I outlined above. We’ll continue monitoring.
I plan to increase my food consumption -- how much do you think I should be eating? I am 6'2", 175 lbs., and rather active (lift 6 days a week, cardio 2 days, 10K+ steps every day). He recommended 3500/day, but that seems like an extreme leap to me.
Final note: he didn’t think I necessarily needed more bloodwork now (as opposed to in 6 weeks), but I asked for it. Thus, I will have a CBC and CMP now. As I understand it, these tests should comprise HCT, HGB, and RBC, among other variables. He wasn’t super concerned about HCT because my level has been quite stable throughout treatment on the four tests I’ve had (45, 46.6, 44, 45.7). But it will be interesting to see how much it has jumped up, given the rise in Free T.
My follow-up with my provider today went well. We are going to lower my dosage from 200mg/week to 180/week; switch from 2X/week injections to 3X/week; and aim to lower estrogen by increasing Danazol dosage. Further, I need to continue monitoring T3 and increase my caloric consumption.
He wasn’t overly concerned about the high numbers. Right now, my Free T is 54.3 (using the decimal-point conversion system), and we are hoping to see it around 40 next time around. We are also hoping to see SHBG go down more and E go down.
Our meeting largely focused on estrogen. He says our goal is to get the E number to be lower than the SHBG number.
He gave me the flexibility to decide how much to increase my Danazol dosage and was happy to go up to 25 mg ED (previously: 25 mg EOD). I’m hoping for some insight here. I was thinking I would do 25 mg 5X/week. My goal is to get SHBG under 50 (was 72 on these recent bloods after starting at 180 at the beginning of HOT). How much would you increase it? Would you go up to 25 mg ED? I do not want to employ an AI, though I do have some on hand if needed.
It seems Danazol will intermittently be a part of my protocol for the foreseeable future. Once we get SHBG sufficiently low — which will allow me to have a more moderate T level — we will lay off the Danazol for a while, then reintroduce it if SHBG increases too much. This cycling system will be in place to reduce the risk of liver toxicity. That liver toxicity possibility is why I'm not ruling out an AI entirely. It may need to come into play at some point.
We also talked a lot about my high Reverse T3. He believes this is a result eating too few calories — something he sees a lot in bodybuilders who do caloric restriction. He believes I should be eating a lot more (currently: all the way down to 1800 cals, as I have been cutting for 2 months). My T3 is now 9% of my Reverse T3, and our goal is for it to be 20% or more. But raising thyroid hormones can also raise SHBG, so we are going to leave this alone for now and just roll with the other changes I outlined above. We’ll continue monitoring.
I plan to increase my food consumption -- how much do you think I should be eating? I am 6'2", 175 lbs., and rather active (lift 6 days a week, cardio 2 days, 10K+ steps every day). He recommended 3500/day, but that seems like an extreme leap to me.
Final note: he didn’t think I necessarily needed more bloodwork now (as opposed to in 6 weeks), but I asked for it. Thus, I will have a CBC and CMP now. As I understand it, these tests should comprise HCT, HGB, and RBC, among other variables. He wasn’t super concerned about HCT because my level has been quite stable throughout treatment on the four tests I’ve had (45, 46.6, 44, 45.7). But it will be interesting to see how much it has jumped up, given the rise in Free T.
madman
Super Moderator
[QUOTE="madman, Im confused right now, from what i've been reading the last few months is that high SHBG is a problem and goes hand in hand with low FT, the reason that men with elevated shbg have high T is that the testicels keep trying to make up for the lack of available T? Is this completly wrong or? Me 118 SHBG. And walking around with severe complaints that all fall in line with low T.
high SHBG is a problem and goes hand in hand with low FT
- most definitely but you need to understand that ones FT levels not only depend on just ones SHBG level but most importantly what TT levels one has.
- in general when one has low TT or sub-par TT levels it is a given that one will have low/sub-par FT levels
- in cases of high SHBG most will have a descent TT 600-700 ng/dL but in many cases will have low/sub-par FT and depending on how high SHBG is.....the higher the level the lower one FT will be for the same TT......meaning if you take one man with a TT of 600 ng/dL and SHBG of 50 nmol/L and you compare it to another man with the same TT of 600 ng/dL but a higher SHBG of 90 nmol/L than the latter person will have a lower FT level for the same TT level.
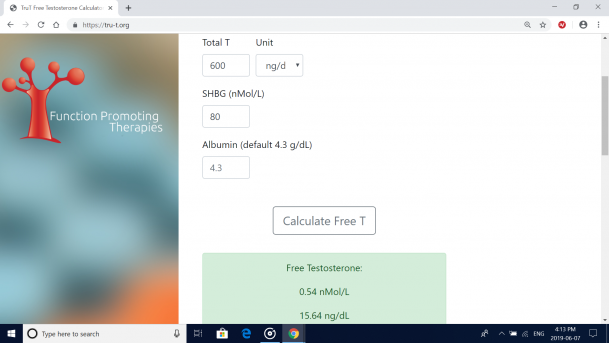
If we use the newer calculated method TruT Free Testosterone Calculator by FPT
Than if one had a TT 600 ng/dL, SHBG 50 nmol/L and Albumin 4.3 g/dL (mean) than FT would be 18.51 ng/dL (low end of the reference range 16-31 ng/dL)
If the other person had the same TT 600 ng/dL, but a higher SHBG 90 nmol/L and Albumin 4.3 g/dL than FT would be 14.76 ng/dL (LOW) reference range 16-31 ng/dL
So as you can see even with both men having a descent TT of 600 ng/dL one will have sub-par FT (low end reference range) and the other will have low FT (below reference range).....due to the difference in the SHBG levels (both are high but one is clearly a lot higher) and although there is a big difference in SHBG levels 50/90 nmol/L (40 nmol/L) you will notice that FT levels are not as drastically different 18.51/14.76 ng/dL even though both men have the same descent TT level.....due to the complex, non-linear allostery in SHBG's association with testosterone.
Even with an SHBG of 70,80,90,100 as long as TT is high enough one can have a healthy FT......but even then TT will not need to be as high as we used to think due to the complex, non-linear allostery in SHBG's association with testosterone.
Attachments
Last edited:
madman
Super Moderator
@madman
My follow-up with my provider today went well. We are going to lower my dosage from 200mg/week to 180/week; switch from 2X/week injections to 3X/week; and aim to lower estrogen by increasing Danazol dosage. Further, I need to continue monitoring T3 and increase my caloric consumption.
He wasn’t overly concerned about the high numbers. Right now, my Free T is 54.3 (using the decimal-point conversion system), and we are hoping to see it around 40 next time around. We are also hoping to see SHBG go down more and E go down.
Our meeting largely focused on estrogen. He says our goal is to get the E number to be lower than the SHBG number.
He gave me the flexibility to decide how much to increase my Danazol dosage and was happy to go up to 25 mg ED (previously: 25 mg EOD). I’m hoping for some insight here. I was thinking I would do 25 mg 5X/week. My goal is to get SHBG under 50 (was 72 on these recent bloods after starting at 180 at the beginning of HOT). How much would you increase it? Would you go up to 25 mg ED? I do not want to employ an AI, though I do have some on hand if needed.
It seems Danazol will intermittently be a part of my protocol for the foreseeable future. Once we get SHBG sufficiently low — which will allow me to have a more moderate T level — we will lay off the Danazol for a while, then reintroduce it if SHBG increases too much. This cycling system will be in place to reduce the risk of liver toxicity. That liver toxicity possibility is why I'm not ruling out an AI entirely. It may need to come into play at some point.
We also talked a lot about my high Reverse T3. He believes this is a result eating too few calories — something he sees a lot in bodybuilders who do caloric restriction. He believes I should be eating a lot more (currently: all the way down to 1800 cals, as I have been cutting for 2 months). My T3 is now 9% of my Reverse T3, and our goal is for it to be 20% or more. But raising thyroid hormones can also raise SHBG, so we are going to leave this alone for now and just roll with the other changes I outlined above. We’ll continue monitoring.
I plan to increase my food consumption -- how much do you think I should be eating? I am 6'2", 175 lbs., and rather active (lift 6 days a week, cardio 2 days, 10K+ steps every day). He recommended 3500/day, but that seems like an extreme leap to me.
Final note: he didn’t think I necessarily needed more bloodwork now (as opposed to in 6 weeks), but I asked for it. Thus, I will have a CBC and CMP now. As I understand it, these tests should comprise HCT, HGB, and RBC, among other variables. He wasn’t super concerned about HCT because my level has been quite stable throughout treatment on the four tests I’ve had (45, 46.6, 44, 45.7). But it will be interesting to see how much it has jumped up, given the rise in Free T.
What is of critical importance here is that you are using Danazol to lower your SHBG......there is absolutely no need for extremely high androgen levels 1500+ ng/dL......let alone 2000-3000 ng/dL (ridiculous) not only for one with an SHBG level of 72 nmol/L but it would be a ridiculous level of TT/FT for one with an SHBG of not only 80+ nmol/L but even the absurdly high 200 nmol/L!
Lets take your TT 2889 ng/dL, for shits sake an absurdly high SHBG of 200 nmol/L and Albumin 4.3 g/dL than your FT still insanely high at 84.19 ng/dL (extremely high above the reference range 16-31 ng/dL)
Again most men do well having FT levels in the 25-30 ng/dL range and yes some need to run levels in the 30-50 ng/dL range but not everyone would need to run these levels let alone some could not tolerate very high FT levels.
The TT levels you are running 2889 ng/dL even with an SHBG of 72 nmol/L (recent level) have your FT levels extremely high 103.27 ng/dL
Even with your previous SHBG level of 180 nmol/L running the same TT 2889 ng/dL would still have your FT levels absurdly high 87.02 ng/dL.
When on trt most depending on ones SHBG whether (low/high) have most men running TT levels 800-1200 ng/dL (mind you some men are hitting 1200-1500 ng/dL levels) which would result in FT levels in the 30-50 ng/dL range.
No one on trt would need FT levels 60+ ng/dL for a protocol to be effective.
Running TT levels 2500-3000+ ng/dL are steroid levels which would result in FT levels 80-100+ ng/dL.
As I stated if anything with an SHBG of 72 nmol/L you could get away with running a TT of 1000 ng/dL and your FT would be 31.07 ng/dL (top end of the reference range 16-31 ng/dL)
If your goal is to have FT levels in the 40 ng/dL range than with an SHBG of 72 nmol/L you would only need to run a TT level of 1250 ng/dL and your FT would be 40.51 ng/dL (over the top end of the reference range 16-31 ng/dl)
lower my dosage from 200mg/week to 180/week
- smart move but you may very well need to lower dose further depending on what TT/FT levels you hit on such dose and whether SHBG levels decrease further or stay the same.
He wasn’t overly concerned about the high numbers. Right now, my Free T is 54.3 (using the decimal-point conversion system), and we are hoping to see it around 40 next time around.
-short term there will be no major issues but again he should be concerned that your TT/FT levels are absurdly high (definitely not trt levels) and as far as "Right now, my Free T is 54.3 (using the decimal-point conversion system)".....this is the wrong approach as it is not giving you a true picture of where your FT levels truly sit and the only way you would know is by either having FT tested using the gold standard Equilibrium Dialysis or the Ultrafiltration method or simply using the newer calculated method TruT Free Testosterone Calculator by FPT.....unfortunately your FT levels are absurdly high 103.27 ng/dL (double) of what he states......hence your piss poor treatment.
-this is why it is critical to use the proper testing method for free testosterone as it is critical to truly know where ones levels sit on such protocol
The TruT™ algorithm improves the accuracy of free-T calculations, reducing the potential for misdiagnosis, and better informing providers when designing treatments.
My goal is to get SHBG under 50 (was 72 on these recent bloods after starting at 180 at the beginning of HOT).
- even if your SHBG never budged and stayed around 72 nmol/L as I stated before hitting a TT of 1000 ng/dL would put your FT level at 31.07 ng/dL (top end of the reference range 16-31 ng/dL) and if you ran a TT of 1250 ng/dL it would put your FT levels at 40.51 ng/dL (over the top end of the reference range 16-31 ng/dL).....so regardless your FT levels would be the same as one with an SHBG of 50 nmol/L running a TT of 935/1180 ng/dL
- as you can clearly see using the newer calculated method even when taking one with high SHBG levels whether 50 nmol/L or 72 nmol/L (22 nmol/L difference) one would not need to run a drastic difference in TT levels (TT 1250/1000, SHBG 72 vs TT 1180/935 SHBG 50) would result in similar FT levels due to the complex, non-linear allostery in SHBG's association with testosterone
- * this is key
- The TruT™ calculator provides the ideal solution by using measurements of total testosterone, SHBG, and albumin to calculate free testosterone while taking into account the complex, non-linear allostery in SHBG's association with testosterone. TruT™ is the only calculator available that uses this more complex formulation. References
Improved TruT™ Companion Diagnostics
Based on the fundamental discovery of testosterone partitioning, our team has developed an accurate free testosterone determination method. While examining the mechanistic origin of this systematic inaccuracy in free testosterone values using the linear model of SHBG:testosterone association, we discovered that the SHBG dimer exhibits conformational allostery in binding testosterone. Our TruT™ companion diagnostic, incorporating the correct parameters and non-linear dynamics in T:SHBG association has resulted in a framework for accurate determination of free testosterone values.
The TruT™ algorithm improves the accuracy of free-T calculations, reducing the potential for misdiagnosis, and better informing providers when designing treatments.
People thinking that one with high SHBG needs to run extremely high supra-physiologicals TT levels to overcome SHBG are sorely misunderstood!
Once we get SHBG sufficiently low — which will allow me to have a more moderate T level — we will lay off the Danazol for a while,
- again even with your SHBG levels at 72 nmol/L you would not need to run an extremely high TT level to achieve a healthy FT level
- TT of 1250-1000 ng/dL would have your FT levels in the 30-40 ng/dL range
- even if you drive your SHBG down to 50 nmol/L running a TT of 1180/935 would result in a FT level in the 30-40 ng/dL range
bodybuilders
- definitely sounds as if your doctor treats a lot of bodybuilders as your TT levels are ridiculous for one running trt even with having high SHBG
he didn’t think I necessarily needed more bloodwork now (as opposed to in 6 weeks), but I asked for it.
-if you have already been on your protocol for 6-8 weeks than at the very least one should have TT (LC/MS-MS)/FT (Equilibrium Dialysis or Ultrafiltration or the newer calculated method TruT Free Testosterone Calculator), e2 (LC/MS-MS), Chemistry panel and CBC done.
- Chemistry panel will include lipids as high levels of T can lower ones HDL and CBC will include hemoglobin/hematocrit/RBC's which are critical to keep an eye on when using testosterone
- an increase in T will result in an increase in hemoglobin/hematocrit/RBCs
wasn’t super concerned about HCT because my level has been quite stable throughout treatment on the four tests I’ve had (45, 46.6, 44, 45.7). But it will be interesting to see how much it has jumped up, given the rise in Free T
- you are using injections now and not only are your TT levels extremely high (well into the supra-physiological range) but more importantly your FT levels are way too f***ing high.....most likely your hemo/hemato/RBCs have increased
Attachments
Last edited:
madman
Super Moderator
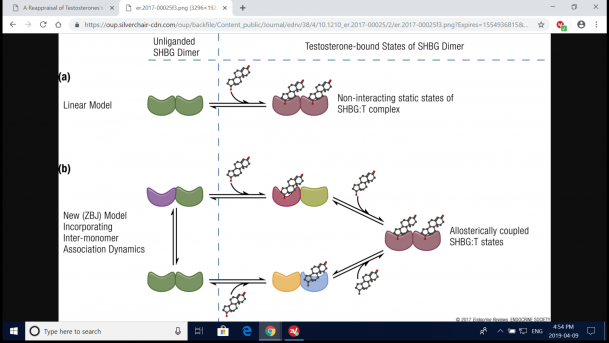
Schematic representation of experimental models of testosterone binding to SHBG. (a) Linear model of testosterone (T) binding to SHBG as conceptualized by Vermeulen et al. (3), Södergard et al.(4), and Mazer (5). (b) New model (ZBJ, schematic adaptation) proposed by Zakharov et al. (34) incorporating the dynamics of allosteric regulation in testosterone binding to SHBG. The different shapes represent conformationally distinct states of SHBG in the dynamic repartitioning of free testosterone into bound forms. Recent evidence derived from new biophysical techniques indicates that the binding of testosterone to SHBG is a dynamic, multistep process. The binding of one molecule of testosterone to the first binding site on an SHBG dimer leads to conformational rearrangement and allostery between the two binding sites, such that the second testosterone molecule binds to the second binding site with a different binding affinity; there is readjustment of equilibria between these interconverting microstates. This multistep, allosteric model provides validated estimates of free testosterone, which have close correspondence with values measured using equilibrium dialysis.
Attachments
After my most recent round of bloodwork, I was curious where some longevity biomarkers were sitting, so I asked for follow-up tests. I had them done Monday and just got the results:



The key numbers — HCT is midrange and has not changed significantly (45.7-46.3); same for HGB (15.5-15.6); and same for RBC (5.19-5.20).
However, I have seen notable changes in ALT (34 in February, shortly after I first started TRT, and now 61) and AST (33 in February, 62 now). Additionally, ALP has dropped from 48-36. I don’t know anything about these biomarkers. Anyone here who can speak to the implications of these results — something to be concerned about?
As a reminder, my T numbers exploded on my last bloodwork. Total T shot up to 2889, with Free T at 543.1. The ratio of Free:Total T was significantly better than what I’d seen before — an encouraging sign — but I lowered my dose (from 200-180/week) because of warnings about the sky-high T levels and how those may harm my long-term health. I also increased Danazol from 25 mg EOD to 25 mg ED (SHBG was still somewhat high at 72).
Given these new results, do you think I should stick with that plan moving forward? I am very happy to see the HCT/HGB/RBC numbers, but not sure how to feel about ALT/AST/ALP.
EDIT: I've learned workout timing affects liver enzymes. I had these tests conducted at 8 a.m. Monday, did an hour of intense cardio on Sunday evening (6 p.m.), and lifted hard (back) on Saturday afternoon.
The key numbers — HCT is midrange and has not changed significantly (45.7-46.3); same for HGB (15.5-15.6); and same for RBC (5.19-5.20).
However, I have seen notable changes in ALT (34 in February, shortly after I first started TRT, and now 61) and AST (33 in February, 62 now). Additionally, ALP has dropped from 48-36. I don’t know anything about these biomarkers. Anyone here who can speak to the implications of these results — something to be concerned about?
As a reminder, my T numbers exploded on my last bloodwork. Total T shot up to 2889, with Free T at 543.1. The ratio of Free:Total T was significantly better than what I’d seen before — an encouraging sign — but I lowered my dose (from 200-180/week) because of warnings about the sky-high T levels and how those may harm my long-term health. I also increased Danazol from 25 mg EOD to 25 mg ED (SHBG was still somewhat high at 72).
Given these new results, do you think I should stick with that plan moving forward? I am very happy to see the HCT/HGB/RBC numbers, but not sure how to feel about ALT/AST/ALP.
EDIT: I've learned workout timing affects liver enzymes. I had these tests conducted at 8 a.m. Monday, did an hour of intense cardio on Sunday evening (6 p.m.), and lifted hard (back) on Saturday afternoon.
Last edited:

Sponsors









Online statistics
- Members online
- 6
- Guests online
- 4
- Total visitors
- 10
Totals may include hidden visitors.

© Copyright 2020 ExcelMale